Designing as Negotiating Across Logic Multiplicity: The Case of Mental Healthcare Transformation Toward Co-design and Co-production
Daniela Sangiorgi 1,*, Josina Vink 2, Michelle Farr 3,4, Gillian Mulvale 5, and Laura Warwick 6
1 Dipartimento di Design, Politecnico di Milano, Milan, Italy
2 Oslo School of Architecture and Design, Oslo, Norway
3 The National Institute for Health Research Applied Research Collaboration West (NIHR ARC West) at University Hospitals Bristol and Weston NHS Foundation Trust, Whitefriars, Lewins Mead, Bristol, UK
4 Population Health Sciences, Bristol Medical School, University of Bristol, UK
5 Department of Health Policy and Management, DeGroote School of Business, McMaster University, Hamilton, Canada
6 Northumbria School of Design, Northumbria University, Newcastle, UK
Designing within complex service systems implies navigating across a plurality of norms and beliefs that multiple stakeholder groups uphold, designers included. Transformational processes may be challenged by minimum, moderate, or extensive conflict depending on the centrality or compatibility of competing logics. This article reflects on how the complexity inherent in higher level institutional orders of society can support or inhibit the potential of co-design in complex systems, particularly in the public sector. Using the context of public mental healthcare transformation as a backdrop, we identified and reflected on four predominant logics: the logic of state; the logic of market; the logic of profession; and the logic of community. We then developed a set of tools to support reflexivity—the excel Logic Multiplicity Workbook and the Layers of Logics Map—that can be used to take project logics snapshots to represent the perceived strength of project stakeholder logics at the micro, meso, and macro levels and their centrality and compatibility. Three co-design project examples were used to retrospectively develop and refine these tools, and support the process of making explicit the role of competing logics in project challenges or triumphs. While we acknowledge that logics are often highly institutionalized and difficult to become aware of, we value as fundamental the creation of tools to better enable designers to consciously adopt adequate strategies to navigate this complexity.
Keywords – Co-design, Mental Health, Logic Multiplicity, Co-Production Regimes, Institutional Logics.
Relevance to Design Practice – This article offers reflexivity tools to designers working in transformational projects within complex service systems to enhance their awareness of the existence and implications of logic multiplicity across multiple stakeholder groups and system levels, to assist in devising design and implementation strategies.
Citation: Sangiorgi, D, Vink, J., Farr, M., Mulvale, G., & Warwick, L. (2022). Designing as negotiating across logic multiplicity: The case of mental healthcare transformation toward co-design and co-production. International Journal of Design, 16(1), 35-54. https://doi.org/10.57698/v16i1.03
Received October 30, 2022; Accepted March 24, 2022; Published April 30, 2022.
Copyright: © 2022 Sangiorgi, Vink, Farr, Mulvale, & Warwick. Copyright for this article is retained by the authors, with first publication rights granted to the International Journal of Design. All journal content is open-accessed and allowed to be shared and adapted in accordance with the Creative Commons Attribution-NonCommercial 4.0 International (CC BY-NC 4.0) License.
*Corresponding Author: daniela.sangiorgi@polimi.it
Daniela Sangiorgi is Associate Professor at the Department of Design and head of the Product Service System MSc at the School of Design of Politecnico di Milano. She is one of the first scholars to work on the application of design for services and service innovation. Her research focuses on innovation in the public sector and health care, with a specific focus on mental healthcare transformation. She has recently become interested in the potential of design toward the transformation of wider care ecosystems. She has published in journals such as Design Journal, International Journal of Design, Design Studies, and Journal of Service Research.
Josina Vink is Associate Professor of Service Design at the Oslo School of Architecture and Design (AHO) and Design Lead within the Center for Connected Care (C3) in Norway. Josina’s research focuses on designing for and within the transformation of healthcare systems and building a systemic understanding of service design. They have published in journals such as Design Studies, Design Journal, Journal of Service Management, and Journal of Service Research. Josina has over a decade of experience working as a service and systems designer in health and care systems in Canada, the United States, and Sweden.
Michelle Farr is a Research Fellow at the National Institute for Health Research Applied Research Collaboration West (NIHR ARC West) and Bristol Medical School at the University of Bristol. She specializes in participatory research methods, co-production, and co-design approaches. She has managed different co-production projects, working alongside members of the public who experience severe health inequalities, to improve health services. She has an interdisciplinary background, having worked across health services, sociology, social policy, and public services management. All her research projects have been in collaboration with non-academic organizations, including a wide range of health and mental health services, local government, and third sector organizations.
Gillian Mulvale is Associate Professor Health Policy and Management and Associate Dean Graduate Studies and Research at DeGroote School of Business, McMaster University. Gillian is health research methodologist (PhD), with a background in economics (BA, MA). Gillian’s research investigates how people with mental health problems and illnesses and other stakeholders can draw on their collective experiences to co-design improved mental health and well-being services and systems. Her recent research program adopts co-production and co-design approaches involving policy-advisors, health system managers, patients/service users, family/caregivers, and other stakeholders working together to improve service experiences, and refines these methods to be inclusive of equity-deserving groups whose participation might otherwise be prohibited by structural barriers. Previously, as Senior Policy Advisor at the Mental Health Commission of Canada, Gillian co-led national consultations involving multiple perspectives (children, caregivers, seniors, Indigenous, service systems, workplace, legal, and science) to inform the goals for Canada’s mental health strategy.
Laura Warwick is a Senior Lecturer in Service Design and Social Innovation at Northumbria University. She extensively researches the impact of Service Design on Voluntary Community Sector (VCS) organizations. Through collaborative projects with local, national and international charities and funders, Laura is able to build an evolving picture of Service Design’s best practice in this context.
Introduction
Co-design approaches are increasingly being applied within organizations and community-based initiatives to inform the transition toward a more human-centered and collaborative design culture or mindset (Julier, 2006). Studies have been exploring how the creation of innovation labs, intended as experimental safe spaces in public service organizations or government, can inform citizen-centric policies and innovation practices (Tõnurist et al., 2017); also, how the establishment of in-house design functions can create design capabilities in staff to support a new way of working (Bailey, 2012; Pierri et al., 2016; Kurtmollaiev et al., 2018).
Regardless of approach, acknowledging existing logics and the organizational context is viewed as fundamental when approaching transformational change processes (Junginger, 2015). This becomes even more relevant when design works within complex service systems that require interaction, or even collaboration, across multiple and diverse stakeholder groups. Not only does each organization have multiple logics, but also external collaborators might introduce different perspectives and fundamental assumptions. This is particularly acute in public service systems where organizations draw on field-level institutional logics (Fligstein & McAdam, 2012) prevalent in both the public and private sectors simultaneously. Furthermore, designers themselves adopt and can reinforce specific worldviews that might clash with multiple logics upheld by those they are working with.
Recognizing and navigating this complexity, while enhancing individual and collective reflexivity, is becoming a fundamental skill for design professionals. However, it is an under-researched area with little discussion of the implications that these conflicting logics and worldviews have on a designer’s attempt to facilitate mutual understanding. Moreover, there is limited understanding of how a designer’s own worldview can reinforce particular logics, thus potentially increasing rather than minimizing conflict.
This paper aims to surface these potential conflicts between logics to reflect on the design implications. It uses the particularly complex context of public mental healthcare transformation with its recent emphasis on recovery-oriented services and co-production, to extract some of the key lessons for designers, and propose a tool for reflection. Mental health systems are particularly revealing contexts in which to examine competing logics because mental health rests at the intersection of many sectors, services, cultures, and communities, and there are often significant tensions arizing when doing co-design (Sangiorgi et al., 2019).
By co-design, we refer to “collective creativity as it is applied across the whole span of a design process” (Sanders & Stappers, 2008, p. 6). This is in contrast to co-production, which we use in this article to refer specifically to the joint delivery of services (McMullin, 2020). Mental health and illness can itself be defined in diverse and competing ways, with different professional and cultural understandings of what constitutes a mental health crisis; for example, the traditional wisdom within Indigenous cultures often contradicts modern views (Borges & Tomlinson, 2017).
In the following sections, we review the meaning of logics and how they are applied to problematize the introduction of co-production in public services and in particular in the case of mental healthcare transformation; we then consider how designing might enact or embody different logics, reinforcing or counterbalancing other perspectives in the field. Conceptual tools—the Logic Multiplicity Workbook and the Layers of Logics Map—are introduced to reflect on the implications of designing with, and at the intersection of these forces, at different levels of a service ecosystem, using concrete project experiences to reveal the resulting power and implementation dynamics. Implications for design research and practice will then be discussed in the closing section.
Introduction to Logics
Discussions around logics have been important for understanding the plurality of norms and beliefs at play and the sources of conflict within situations (Cloutier & Langley, 2013). In this paper, we integrate discussions about logics from a number of discourses, for example: organizational studies; public services; design; and co-production. We use the term logics in this paper to refer broadly to any established set of organizing principles or underlying rationale used to make inferences within different social domains. Logics are the frame of reference that enable people to make sense of the world and their own identities; they shape individual and organizational practices through guiding expectations for social relationships and behavior (Goodrick & Reay, 2011).
Such logics can exist across an entire sector in society (Friedland & Alford, 1991) or rest more narrowly at the field-level, among a group of professionals or within a more limited domain (Goodrick & Reay, 2011). In this way, logics can be more or less institutionalized, with highly institutionalized logics being significantly more enduring, wide-spread, and largely taken for granted (Greenwood et al., 2017). It is also important to note that logics are socially constructed, in that they are enacted by people together, and are not simply cognitive but include sets of material practices and actions (Thornton et al., 2012). They also exist at a macro level, setting the policies, use of resources, and roles of an organization, at the meso level in single or multiple organizations, and at a micro level, shaping the actions of individuals.
In the early discussion of logics, there tended to be a focus on one overriding, dominant logic guiding people’s actions (Prahalad & Bettis, 1986). Later, it was recognized that the coexistence of potentially contradictory logics is the basis of ongoing societal transformation (Friedland & Alford, 1991). The focus in the literature then shifted toward examining the interplay between two competing logics within a particular context, or the shift from one particular logic to another (e.g., Thorton & Ocasio, 1999). More recently, the emphasis has been on the ongoing interplay of multiple logics, constellations of logics, or institutional complexity, to understand the positioning and relation between a larger number of different rationales (Goodrick & Reay, 2011; Greenwood et al., 2011).
For this reason, there is an ongoing debate about how individual organizations need to address multiple institutional demands, and how this manifests in the form of multiple internal logics (Besharov & Smith, 2014). While some studies report on the conflict between these multiple logics, which can diminish innovation potential, others suggest the possibility of a coexistence or a merging of logics (Jaakkola et al., 2019). However, the implications of logic multiplicity depend on how multiple logics are instantiated within organizations (Besharov & Smith, 2014) and how consistent and reinforcing these instantiations are on the organizational actions (compatibility), or how and if they are equally valid to core organizational functioning (centrality). Drivers for higher or lower levels of centrality and compatibility operate at the macro, meso, and micro levels, leading toward different types of logic multiplicity and conflict within specific domains, such as: contested organizations, where multiple logics with limited compatibility vie for dominance offering inconsistent guidance for action; estranged organizations, where a dominant logic is at odds with subsidiary ones generating moderate conflicts; aligned organizations, where multiple logics offer consistent organizational goals and values resulting in minimal conflict; and dominant organizations with a prevailing logic and compatible subsidiary ones coexisting with no conflicts (see Figure 1).
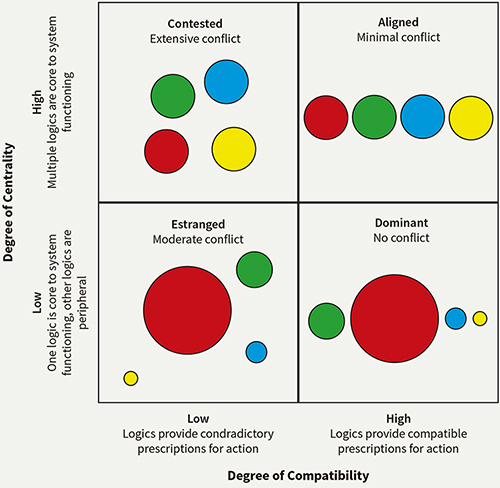
Figure 1. Types of logic multiplicity. Different logics represented by different colours. Adapted from Besharov and Smith (2014).
In contexts where design approaches are introduced to enact transformational change, in effect, designers are attempting to: replace existing institutional logics with another; merge aspects of diverse logics; or remove logics from a common origin (Kurtmollaiev et al., 2018). They are also attempting to do this at both the meso and micro levels, changing the intentions of the organization and the actions of the individuals. Some scholars suggest that multiple logics and institutional complexity can become a toolkit; a set of cultural norms, meanings, and material practices belonging to different institutional arrangements that can become available for creative re-constructions in service innovation (Siltaloppi et al., 2016). However, in order for designers and participants in co-design processes to use logic multiplicity intentionally as a toolkit, there is a need to develop greater awareness of the different logics at play and their manifestations within a given context. In what follows, we examine some of the relevant logics within the public realm and the mental health system as an example to help contextualize what it means to design within logic multiplicity.
Logics in the Public Service Realm
In the public sector, conflicting logics have been associated with different governance paradigms that imply a gradual transformation in the conception of the relationship between the government and citizens. The Public Administration model, largely based on top-down bureaucratic monopolies with public service users as passive recipients, was gradually contested in the 80s and 90s in favor of an approach inspired by the private sector where citizens were described as customers in demand for personalized and efficient services (Dunleavy & Hood, 1994). Lately, there has been a move away from the New Public Management model (NPM), in favor of the New Public Governance (NPG) paradigm (Osborne, 2010), also called Network Governance (Kelly et al., 2002) or Digital Governance Model (Rainford & Tinkler, 2011). The NPG paradigm is introducing a more co-operative form of governing that substitutes the focus on responsiveness to customers’ needs, with an emphasis on power sharing and collaboration between governments and citizens. Recently, a Communitarian (mixed) model has been added, completing the picture of co-production regimes (Pestoff, 2018) that actually still coexist in our welfare systems.
The co-existence of these evolving policy ideas and modes of governance can be described as a form of institutional layering, where policy-makers intervene additively to the existing institutional arrangements, in contexts where radical institutional change is not possible or desirable (Capano, 2019). How these policy ideas interplay and become embodied in practices in organizations and professionals, depends on the dominant logic of the institutional field in which they operate (Friedland, 2013). Different sectors can have specific and defining logics, but they are nested within the higher-level institutional orders of society that provide the cultural symbols and material practices that condition as certain areas of life, such as: family; community; religion; state; market; profession; and corporation (Thornton et al., 2012).
It has been discussed how, at meso and macro levels, these orders can support or inhibit the potential and implementation of co-production (McMullin, 2020). As McMullin illustrates (see Table 1), a state logic might, for example, be aligned with co-production in its democratic principles, but could become a barrier when its bureaucracy and risk aversion culture tends to dominate; this might depend on the peculiarity and history of the national culture or the level of government (central vs local) involved. A market logic can instead be associated with NPM, dominated by a focus on performance and efficiency, that might clash with a communitarian logic that instead values long term participatory and community-based approaches. Finally, the profession logic that values individual expertise based on professional training is often conceived as one of the major barriers to co-production. While these four logics and their impact on co-production can be considered as archetypical, they might need further articulation or expansion depending on the context of action.
Table 1. Impact of institutional logic on co-production (McMullin, 2020).
| Logic | Description | Implications for involving citizens in policy implementation (co-production) |
| State | Based on democratic participation, bureaucracy, hierarchy | Viewed as a way to legitimize public policy and democratic ethos OR challenge to equitable distribution of public resources. Government bureaucracy and risk aversion as a barrier. |
| Market | Competition, efficiency, performance management, citizens as consumers | Contract requirements based on cost effectiveness may limit holistic, collaborative approaches. Shift towards personalization/individual co-production rather than collective approaches or more democratic motivations. |
| Community | Trust, reciprocity, solidarity | Explains difference in approach to implementation between public and third sector organizations. Supports relational, collaborative approach between different actors. |
| Professional | Personal expertise based on professional training and experience | Co-production can challenge professional legitimacy–barrier or obstacle for public servants in professionalized sectors. |
As an example, healthcare systems constitute an institutional field, meaning a community of actors that are united by a dominant set of values and beliefs (Scott et al., 2000), such as: purchasers of health; intermediaries; governing bodies; and patient organizations and groups (Currie & Guah, 2007). As it has been the case for the public sector in general, healthcare systems have been living through different eras with different dominant logics, e.g., moving from an era of professional dominance, where clinicians had relative autonomy and freedom and were paid directly by the State, to an era of managerialism and market mechanisms, inheriting models, approaches, and values from the private sector (Currie & Guah, 2007; Reay & Hinnings, 2009). In a study into the context of public healthcare, scholars found that there were four key logics at play: profession (expert care); market (supply and demand); corporate (organizational rules); and state (legislation and rights) (Raey et al., 2017). However, there is also recognition that the relationship between these logics can play out differently across different countries (Waldorff et al., 2013).
In the general shift toward patient centricity, medical professionals are said to operate between conflicting logics, e.g., the science logic and the care logic that have been affecting the alternating forms and content of medical education: “a science logic focuses on knowledge of diseases built through research and innovative treatments, whereas a care logic highlights physicians’ clinical skills used to treat patients and improve the health of the community” (Dunn & Jones, 2010, p. 116). Other scholars suggest that there is a contrast between a logic of choice, from a market-based logic, with the logic of care, an emotional, interpersonal process (Mol, 2008). De Zulueta (2013) also explores different logics within health services, including professional virtues, compassion and contrasting market based NPM, and mechanistic and biomedical paradigms.
While these competing logics might inhibit change and innovation, there is evidence of strategies at the micro level of individuals that can favor a successful coexistence, e.g., developing pragmatic collaborations to achieve a common goal, while maintaining a distinguished set of beliefs and values (Reay & Hinnings, 2009), or the re-definitions of professional identities that combine conflicting logics, e.g., from an identity of an autonomous expert clinician to an informed head of a multidisciplinary team (Reay et al., 2017). In the study of hybrid social enterprises working in the health and social care field, innovative solutions are also considered the result of the coexistence of three competing logics, from the public, the market, and the civil society (Vickers et al., 2017).
The Example of Mental Healthcare
This discussion has wider implications when we move toward co-design and co-production in mental healthcare, as this transformation implies designing in highly contentious areas (Sangiorgi et al., 2019). The push toward the deinstitutionalization of mental health has led to different forms of community-based psychiatry that clearly exemplify the coexistence of co-production regimes, where transformational efforts take different forms and intent. This coexistence can lead to institutional heterogeneity that manages to maintain plurality, decoupling coordination and control functions from everyday practices (Meyer & Rowan, 1977), but in some circumstances conflicts might end up delegitimizing alternative practices. For example, in an ethnographic study about the introduction in Illinois mental healthcare of Medicaid fee-for-service (FFS) system, it was documented how the traditional quality assurance practices have introduced a managerial logic of cost-efficiency, standardization, and accountability. This clashed with the Community Club House communitarian logic, that instead emphasized membership, social connection, collaboration, and self-determination, ultimately leading to the closure of this service model (Spitzmueller, 2018). The focus on cost savings and efficiency can also compete with a profession logic that aims for customized and holistic care, fighting against standardization and quantification as criteria to inform decision making in psychiatric care (Arman et al., 2014). The need for short term and measurable outcomes conflicts with the nature of mental health problems that are chronic, with a “biopsychosocial philosophy of care which emphasises community integration and continual personal growth and awareness, rather than merely the relief of symptoms” (Scheid, 2000, p. 704), generating fundamental ethical dilemmas. The coercive and normative pressure from the State on local mental healthcare providers can generate network-level responses that build on cooperation instead of competition, as in the case of community-based mental health (Provan et al., 2004).
Furthermore, there have been a range of movements in contestation to psychiatric logics and bio-medical models within mental health services. Some movements, such as the anti-psychiatry movement, were led by psychiatrists themselves, e.g., R.D. Laing (Crossley, 1998). Other examples, such as the Hearing Voices Network, were collaborations between psychiatrists and people who can hear voices, who promoted practices that were traditionally antithetical to psychiatric treatment (Garety, 2001). The development of Mad Studies contests both the marketization and medicalization of people’s distress (Beresford, 2016). Institutions such as the British Psychological Society have begun to develop alternative paradigms to understand experiences of mental distress, responding to the reductionist medical approach, with alternative, more trauma-informed approaches (Johnstone & Boyle, 2018). These types of approaches focus on inquiries about what has happened to people, and contest medical approaches that are informed by questions like what’s wrong with you? Survivor movements have been defined by the need for survivors to speak and act for themselves; survivors working with others on equal terms basing their work on lived experience and experiential knowledge (Beresford, 2016). Yet, even survivor social movements have been critiqued as duplicating white privilege, and the whole concept of co-production within mental health services has been contested as an untenable promise (Rose & Kalathil, 2019).
As documented by this short review, multiple competing logics that might support, limit, or co-exist in mental healthcare transformation projects can be experienced by designers during design interventions, acknowledging how culture significantly affects mental health and mental health services in different countries (Gopalkrishnan & Babacan, 2015). Overall, this paper is interested in which strategies designers and design researchers can adopt to reveal and better incorporate these field-level influences, while adopting a Western perspective in the context of North American and European mental health systems. Before doing so, we want to acknowledge how design professionals themselves, as new external actors entering this complex field, might bring and perform other values and material practices that could become aligned, contested, estranged, or dominant in the complex mental healthcare system.
Enacting Logics through Design
In recent literature, design is viewed as a transformative force for changing institutional logics (Kurtmollaiev et al., 2018). It is recognized as a means to shift mental models and disrupt long-held habits, to spark reflection on existing logics and create the potential for change (Vink et al., 2019; Wetter-Edman et al., 2018). However, it is important to recognize that design itself is not neutral and also enacts particular logics (Vink et al., 2019). The co-design process is not separate from the logics existing in different spheres of society but can amplify or undermine these logics enacting or embodying them through the process as discussed in the following subsections, using McMullin’s (2020) archetypical logics.
Design’s Connection to Different Societal Logics
There is a growing body of literature highlighting design’s role in perpetuating a market logic. It is recognized that design has become a profession serving capitalism, which has an underlying logic of exploitation of people and other living things (Willis, 2018). Research on participatory governing processes has illustrated how the “adoption of private sector design discourses and practices into public services follows neo-liberal political trajectories” (Farr, 2019, p. 165). When design moves into public policy-making spaces, such as through prototyping, scholars argue that it can catalyze the further encroachment of market logics into government, absorbing the critiques of capitalism along the way (Kimbell & Bailey, 2017). In this way, design “can downplay challenges to the dominant neo-liberal consensus, dilute differences in political agency, and mask the politics inherent in deciding who, or what, co-emerges within a prototyping assemblage” (Kimbell & Bailey, p. 222). Within a market logic, design explicitly or inadvertently supports commercial outcomes with efficient transactions by creating user-friendly services that drive profits.
Design processes can also enact a profession logic that emphasizes personal expertise in connection to the craft of design. Willis (2018) suggests that our understanding of design is “overdetermined by the model of professional design as the model of all designing” (p. 2). Early literature on design for service reinforces an expert-driven design process, suggesting that “process design is management’s responsibility” (Shostack, 1984, p. 139). Furthermore, many empirical studies focus on the design work of professional consultancies and firms, reinforcing the important role of the design professional (e.g., Zomerdijk & Voss, 2010; Yu & Sangiorgi, 2018). While the design professional is increasingly expanding to include multidisciplinary members (Grenha Teixeira et al., 2017; Joly et al., 2019) and sometimes also includes “selected customers to become members of the service design team” (Trischler et al., 2018, p. 76), design reflects this profession logic and continues to maintain some exclusivity and emphasize expertise.
Sometimes design processes also reflect a state logic connected with democratic participation and redistribution to enable the collective good (Holmlid, 2009). This logic is often driven through the integration of participatory design approaches that have a long history of working to amplify the voices of those affected by a system but marginalized in decision-making, explicitly focusing on re-balancing power (Kensing & Blomberg, 1998). In addition, this state logic is also reflected in design literature that highlights efforts to empower end users and/or staff by engaging their competencies in the process (Hussain et al., 2012; Taffe, 2015; Wetter-Edman, 2012). However, within such co-design processes, design can operate within “politically defined visions of the future” (Bason, 2010, p. 153) rather than challenging institutional power and policy trajectories (Farr, 2013). Furthermore, when taking on a state logic that supports the status of a particular interest group, it is increasingly recognized that it can enact legacies of colonization, controlling ways of knowing and designing (Akama & Yee, 2019; Schultz et al., 2018).
Some intentional design practices also reflect a community logic by actively supporting unity, trust, and cooperation. Such a logic may be enacted when design promotes reciprocal approaches to co-design respecting that design is already located in local practices, including Indigenous ways of knowing and designing (Akama & Yee, 2019). By supporting more autonomous ways of communities designing themselves, rather than imposing one way of doing design or one version of reality, design can embrace plurality and community values through its process (Escobar, 2018), eventually losing control of the output, but valuing the process more. However, when doing co-design in public institutions, “service design practices may aim to improve services for users, but they are not rooted within political movements that contest inequalities, or work toward social justice and democratic rights” (Farr, 2019, p. 165). As such, while a community logic is sometimes enacted, design can also symbolically adopt a community language without fully embracing community ideologies and practices, or working alongside community activists.
The Need to Make Design’s Logics Explicit
Any given design project may vary considerably in terms of its aims, success measures, understanding of systems, and the role of participants, depending on the logics of the context, the approach, and designers. However, as we illustrate below, design is embedded within particular logics and forwards certain values through the transformational projects in which it is involved. Furthermore, within each project, regardless of the logics adopted by the project sponsors or designers, participating stakeholders also hold different logics that shape their participation, expectations of the project aims, and perceptions of the success of outcomes. Designers have the challenging task of managing the expectations of these various groups, while recognizing their potentially different aims, success measures, and understanding of systems. The outcomes of design engagement approaches may therefore be disappointing to participants, and particularly for more marginalized groups seeking to challenge and breakdown existing mental health systems.
Logics are inherently political, and there is growing acknowledgement that design must better attend to the logics it enacts within specific political landscapes. As a carrier of particular logics, design risks othering local and Indigenous knowledge and practices with industrialized, Euro-centric ways of working (Akama & Yee, 2019). In this way, design becomes an ontological instrument that might control and discipline people’s perceptions and interpretations of the world (Tlostanova, 2017), effectively imposing Western logics associated with modernity over others. As such, there are growing calls for design to “acknowledge and pay respect to paths by which ideas, projects, and designs arrive within and relate to particular contexts” (Schultz et al., 2018, p. 2). Remaining attached to a normative understanding of co-designing as inherently good can leave designers unprepared to anticipate or understand emerging logic conflicts (Vink et al., 2017). Conflicts might emerge within design approaches themselves, or when they become a vehicle for wider political strategies and trajectories (Farr, 2019). However, making these conflicts between logics more explicit can help in intentionally navigating the complexity between different logics through design.
Implications of Logics on Co-design In Mental Health
Bringing together the implications societal institutional orders can have on the mental healthcare field and on design work, we can try to reflect on, and sometimes anticipate, some of the conflicts we encounter when co-designing services at different levels of a mental healthcare ecosystem. Table 2 merges considerations from McMullin (2020) (see Table 1) on how society institutional orders can support or inhibit co-production in the public sector, with the specific case of mental health and logics enacted through design informed by a literature review. The potential implications for co-design are derived by applying each logic to co-design and noting potential risks as suggested in the literature.
Table 2. Summary of the influence of archetypical logics on design and co-design interventions.
| Logic | Description | Relevance for the mental health institutional field | Related design mindset | Suggested implications for co-design |
| State | Based on democratic participation, bureaucracy, and hierarchy | Access to healthcare, healthy population, democratic participation; bureaucratic & normative systems of control (Provan et al., 2004; Scheid, 2008) | Participatory design, citizen empowerment, controlled processes and outcomes (Bason, 2010; Kensing & Blomberg, 1998) | Design can reinforce the democratic ethos that supports mental health users & staff participation in co-design, but it is not always disruptive, as it tends to align with current political mandate (Bason, 2010). |
| Profession | Personal expertise based on professional training | Customized, quality holistic care; needs oriented care, autonomy, and decision making; science logic & logic of care (Scheid, 2003) | Value of design professionals, expert-led design processes, multi-disciplinary teams (Shostack, 1984; Willis, 2018) | Design & expert led approaches can favor qualified outcomes, but might limit lay contributions and empowerment, and reinforce power dynamics. |
| Market | Competition, efficiency, performance management, citizens as consumers | Logic of choice, managed care cost-efficiency, standardization, & accountability, focus on quantification (Scheid, 2003) | Marketable outcomes, efficient, user-friendly transactions, profitable approaches (Farr, 2019; Kimbell & Bailey, 2017) | Design can guide toward co-design as an innovative and valuable service model to be scaled up and sustained, but it might lose sight of minority or local objectives. |
| Community | Trust, reciprocity, solidarity | Social value and democratic engagement with employees and service users. Caring for membership, social connection, collaboration, and self-determination (Scheid, 2008; Spitzmuller, 2018) |
Reciprocal approaches, communities designing for themselves, connected to local social movements, time for trust building (Akama & Yee, 2019; Escobar, 2018) | Design can act as a facilitator for community based and collaborative solutions, but with less control on the final output; co-production can be emergent and co-evolving. |
When design is aligned with a state logic, the principles and practices of a participatory approach to design (Kensing & Blomberg, 1998) can reinforce the democratic ethos of co-production in mental health, even if its contribution might not always be disruptive as design tends to adhere to the current political mandate (Bason, 2010). When, instead, design is adopting a profession-centric mindset (Willis, 2018), the value of design expertise and contribution can dominate the design intervention, with the potential consequence of limiting lay contributions, and reinforcing existing power dynamics. If design is more associated with a market logic, efficiency and profitability might dominate its perspective (Farr, 2019; Kimbell & Bailey, 2017), leading toward possibly innovative co-produced service models, but with the risk of losing sight of minorities and their local needs and objectives. Finally, when design embeds a community logic, it is more inclined to acknowledge and support local social movements and expertise (Akama & Yee, 2019; Escobar, 2018), facilitating community-based and collaborative solutions, with potential consequences of losing control of the final output and its actual development.
With these considerations in mind, we reflect on our past projects in mental health to explore if and how these dynamics and implications could be retrospectively recognized and to consider which kind of tool or framework could facilitate this process when designing.
Methodology: Development of the Conceptual Tools
Recognizing the contentious nature of designing for mental health system transformation amid multiple logics (Sangiorgi et al., 2019), the authors of this paper, made up of an interdisciplinary team of researchers, began to reflect on the ways that these logics manifested within ten co-design international projects that we had been involved in. These projects addressed issues such as: digitalization; nurse-patient therapeutic engagement; peer support; co-production; and recovery within mental healthcare systems in Italy, United Kingdom, Canada, and Sweden. Connected with a variety of jurisdictions and populations, these projects targeted changes ranging from within a single service to across multiple organizations, and throughout provincial or national systems, lasting between 8 months to 3.5 years. Using previous comparative work of these ten cases (Sangiorgi et al., 2019), the authors aimed to recollect critical moments when these logics manifested in the form of evident clashes or positive developments and collaboration. Taking an abductive research approach that moves between empirical material and theory (Dubois & Gadde, 2002), we then identified institutional logics as supportive explanatory theory to aid in understanding the dynamics happening within the projects. When applying this theory, it was soon determined that a tool to support the reflection process and to map some of the results could help make the identification of these intricate and often invisible dynamics easier, more rigorous, and accessible for others. Next, we began sketching out possible tools for mapping the multiplicity of logics and exploring their implications, combining the project context and literature on institutional logics. In the process of application to different projects, it became clear that logic multiplicity could manifest differently at the macro (e.g., field or national), meso (e.g., sectoral or organizational), or micro (e.g., group or individual) level, but that these levels were interdependent, often affecting the evolution of one another.
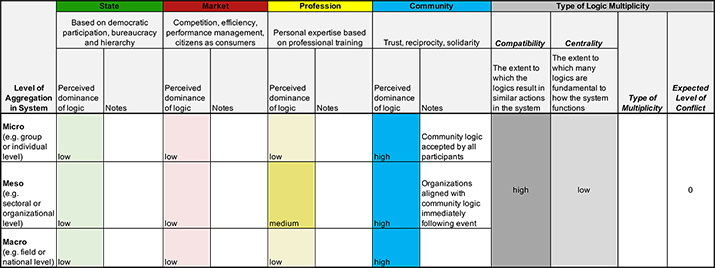
Through ongoing iteration, application, and refining based on both effectiveness and accessibility for use across our project contexts, we developed an excel file and a divided wheel shape with nested circles to reflect on and capture the connections across multiple logics and their multi-level enactments. The excel file and the visual tool were then further refined through an in-depth application of them to three illustrative cases that were selected because of their divergent logic dynamics and different developments and results. In particular, the excel file was used as a workbook to reflect on specific instances of past projects (see example in Figure 2), with columns representing the perceived dominance of logic at different levels of the ecosystem and the overall perceived centrality and compatibility (low or high) of the different logics, inspired by the work of Besharov and Smith (2014). The excel file would then have an automated function, leading to the resulting type of multiplicity and consequent expected level of conflict which have been collapsed to the project level where the implications of these dynamics manifest (see Appendix 1, 2, 3, and 4 for the excel workbook and examples of application).
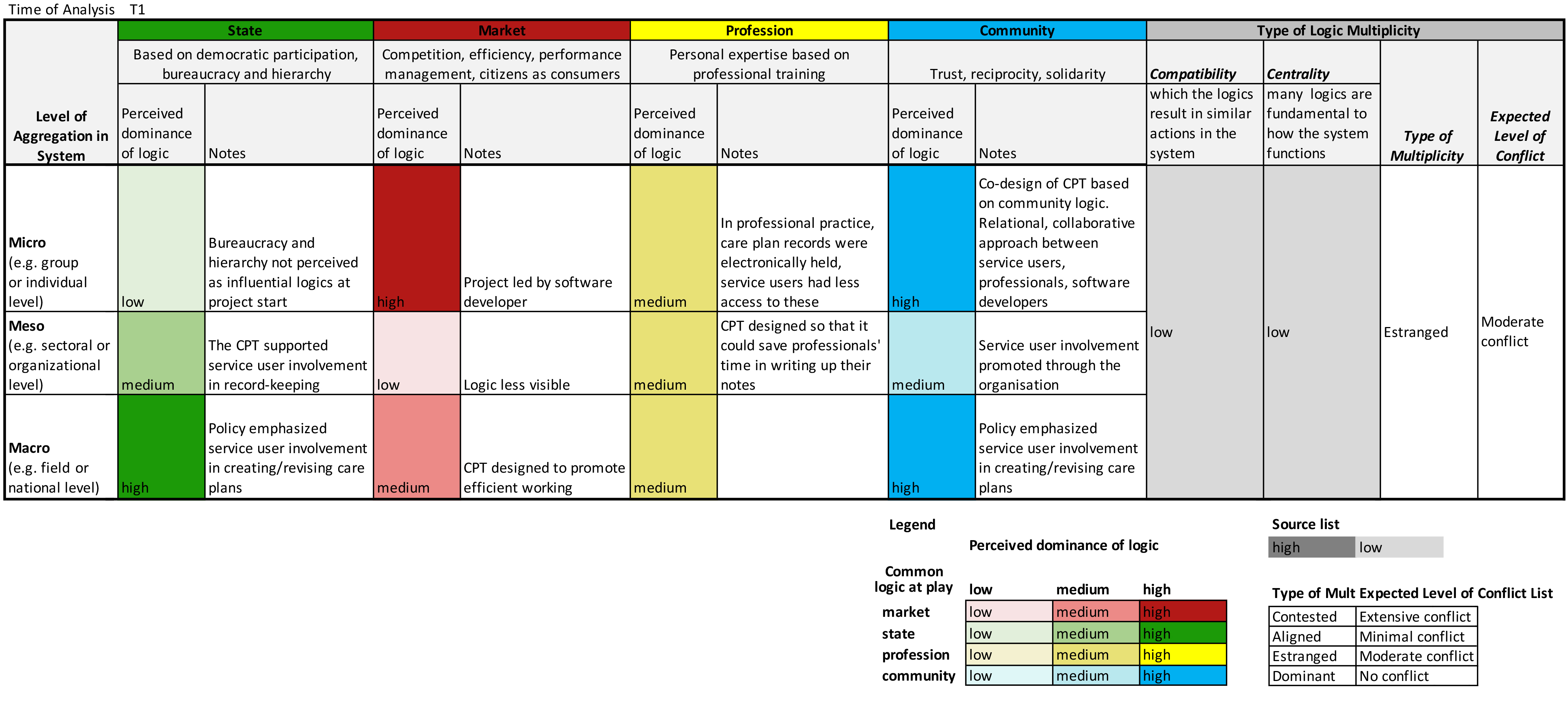
Figure 2. Example of use of the Logic Multiplicity Workbook. (Click on the figure to enlarge it.)
The Layers of Logics Map, instead, shown in Figure 3, would then use what emerged from the workbook, to map and visualize the researchers’ perceived strength of the logics at different levels using different colour intensity, starting from their experience in and research on the mental health design project and supporting materials. As the figure suggests, we can use the wheel moving across different levels of a system, to recognize and reflect on the ongoing encounters or clashes between multiple logics, including the role and logic design plays, that can become evident in specific stages of a project. This wheel was then complemented with maps showing the perceived centrality and compatibility of the different logics, as a way to reflect on the origins of the identified conflicts and particular project developments. In both tools, a color legend was adopted as a way to visualize the evaluation and, later on, make it easier to share and understand the weight and role the logics played in the represented project stage and at the different levels of the system (through a more comprehensive project logic snapshot). In this process, we recognized that this tool aided reflection and supported a more nuanced conversation about logic multiplicity.
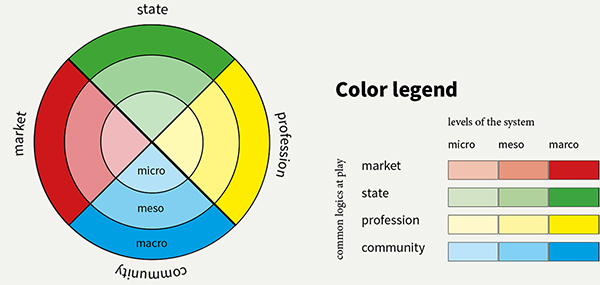
Figure 3. The Layers of Logics Map.
As mentioned above, the wheel was refined and its value demonstrated through application to three divergent examples of co-design projects for mental healthcare transformation that the authors were part of. In what follows, we reflect on which logics manifested in each of the three projects over the course of their development; their perceived strength across the levels; and how this multiplicity might have affected the final result by providing before and after project snapshots using the layers of logics tool. Each of these narratives is crafted through the interpretation of researchers who were involved throughout each of the projects, looking back retrospectively, with input from additional project stakeholders where possible. The intention of these narratives is to contextualize the conceptual discussion above within different project settings and show how these insights relate to design practice.
Project Analysis Examples
Our three examples, described below, are based within the mental health systems of the UK and Canada.
Example 1—Mums Matter
In June 2015, Mind, a federated charity that aims to improve the mental health and wellbeing of people living in England and Wales, embarked on a project to co-design a service for women with poor perinatal mental health (from pregnancy to the child’s first birthday). The result was an eight-week course, Mums Matter, which introduced key content to support service users to manage the everyday, dispel myths, and nurture themselves. The service is currently being delivered by Mind in eight locations across England and Wales. Figure 4 shows a snapshot of the configurations of logics at the beginning and end of the project, as these logics evolved over time.
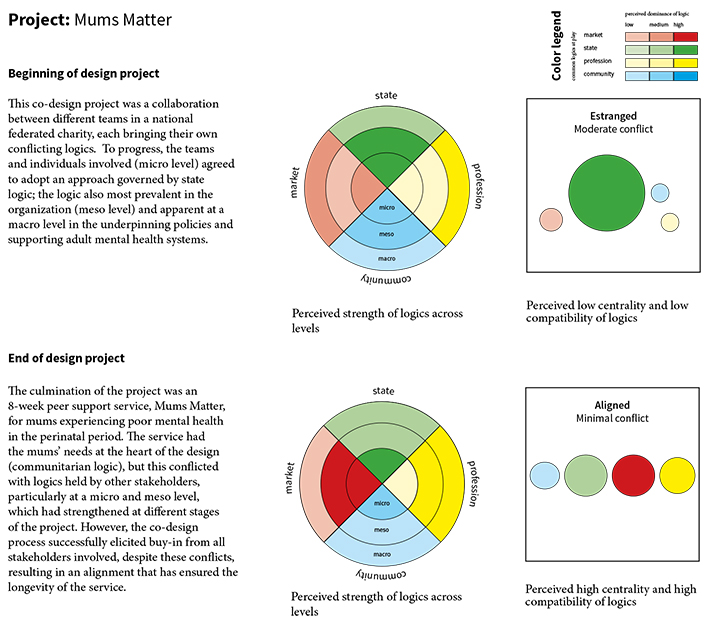
Figure 4. Mums Matter Layers of Logics Map.
At Beginning of Project
The project was run in collaboration between two of Mind’s programmes: Service Design in Mind (SDiM), which supported Mind teams to use service design to develop mental health services (Pierri et al, 2016, p. 580); and the Products programme, which created off-the-shelf packages of fully developed and evaluated services that could be sold to local commissioners. The logics of these two teams were ordinarily combative, as the SDiM team adopted a communitarian logic and the Products team generally brought a market logic to their work. However, the Products team agreed to the participatory, open principles of the design process, and, likewise, the SDiM team had agreed to put boundaries around the potential design solutions; thus, on reflection, they both agreed to temporarily adopt a state logic.
State logic also appears to have matched logics at a meso level; as a large charity, Mind predominantly holds a state logic, but with aspects of community logic as those with lived experience are central in decision-making. At a macro level, the project was partly driven by the commissioning of The Five Year Forward View for Mental Health (Mental Health Taskforce, 2016), which found a lack of specialist perinatal mental health care and outlined a significant investment in local services to address inequalities. As an NHS England initiative, this would ordinarily hold a profession logic. However, the taskforce had taken a person-centred, cross-sector approach, which placed it at the care-end of the profession logic spectrum, thus allowing for alignment with other logics at meso and micro levels of the project.
Logic and Strategies through the Project
The project had a tight timescale, so, in order to avoid any delay, the recruitment process for the co-design team (five mums with lived experience and two local Minds staff who had professional expertise) sought members who aligned with the agreed approach, and thus the dominant state logic. Although the local Mind members undoubtedly brought aspects of a profession logic, it was pre-determined that the mums as “experts on their experience” (Visser et al., 2005, p. 128) would be the key decision makers. This helped to create an inversed power hierarchy, rather than simply a flattened one, enabling the project to continue to progress based on the mums’ consensus. The SDiM team supported the co-designers to go through the key stages of the design process: undertaking primary research; identifying insights; generating ideas; and prototyping key touchpoints. Despite the aligned logics, tensions did still arise when defining the final solution, as it conflicted with one of the mum’s own experiences of care; she had experienced in-patient care, whereas the other four mums had received different types of community-based support. In that instance, the boundaries of the design project as a community-based mental health offer helped to navigate those clashes (Warwick et al., 2018).
At End of Project
The design activity had proceeded without issue, as, on the surface, the meso-level logics matched those of the design approach. However, conflicting logics became apparent when funding was required for the live prototyping stage and some of the Executive Management Team (EMT) questioned the reliability of the service design approach. They drew on the profession and market logics at play within the NHS to question the small sample sizes involved in design projects; they perceived this as a lack of rigour, and thus they lacked confidence that the service would be commissioned. To temporarily align these potentially estranged logics, the design team had to evidence through examples that the approach could produce scalable, sustainable services valued by the public sector. The EMT then sanctioned the funding required for the project to proceed to the next stage. At that point, more evidence of the service’s efficiency and efficacy was gathered to satisfy those logics and ensure the service proceeded to a full pilot.
Example 2—Care Pathway Tool
The macro-level policy context of this example emphasized the involvement of service users in creating and revising their care plans (Department of Health, 2008; Mental Health Taskforce, 2016), which has been shown to support recovery (Bee et al., 2015). However, in professional practice, care plan records are usually electronically held, and service users often don’t have access to these (Brooks et al., 2018). To change this, the software developer Otsuka Health Solutions (which has been acquired by Holmusk) co-designed an electronic care pathway tool (CPT) with service users and staff at a mental health services trust within NHS. Staff used the tool with service users on a touchscreen tablet to support joint working and the co-production of care and crisis plans. An academic study then investigated staff experiences of using the tool with service users in a pilot project, exploring what it was like to use the tool in everyday practice (Farr et al., 2019, Pithara et al., 2020). Figure 5 provides an overview of the logics at the beginning and end of the Care Pathway Tool project. How the dynamics between logics played out in this project is described in more detail in the sections below.
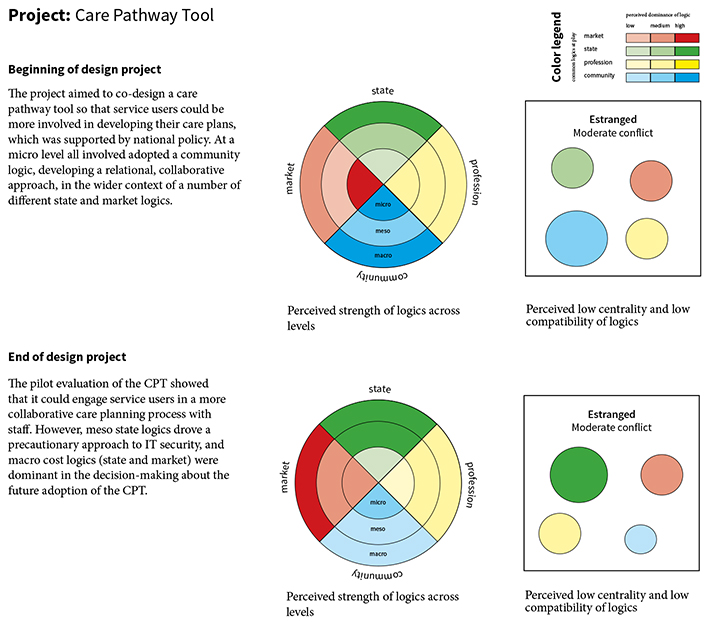
Figure 5. Care Planning Pathway Tool Layers of Logics Map.
Beginning of the Project
At a micro level, the co-design of the CPT was based on a community logic, developing a relational, collaborative approach between different actors (service users, professionals, software developers). This enabled a collective and collaborative co-design process to develop the CPT. In practice, at a project micro level, logics aligned through a pragmatic collaborative aim to co-design and implement a pilot of the care pathway tool (CPT). Service users, clinicians, managers, commissioners, academics, and IT developers met together to co-design, develop, and then implement and evaluate the use of the CPT. To ensure service user involvement was inclusive, service users often met up before these meetings to prepare and support each other, the chairing encouraged participation from everyone, and there was a reflective space during the meetings to support service users’ involvement, which helped to affect involvement culture and practice. This project was supported at a macro level by policies that supported the involvement of service users within mental health services and their care plans. However, the project was placed within a wider set of underlying meso and macro logics which were less visible and apparent at the start, that combined market logics (efficiency, cost-effectiveness) and state bureaucratic logics within NHS institutions.
Logics and Strategies through the Project
The pilot evaluation found that, at a micro level, the CPT could engage service users in a more collaborative care planning process with staff, supporting discussion about people’s support networks, future plans, and what to do when they could see early warning signs of a crisis. Usual practice was for health records to be kept in offices, and for staff to update these records after they had visited service users in the community. Some service users were surprised to hear that these records existed and were keen to take part in writing them. The tool enabled them to take part in this process (Farr et al., 2019). Record-keeping (an enactment of the state & profession logics) was supported by a co-designed electronic tool (community logic) which professionals could also appreciate as it saved them time in writing up their notes. However, there were tensions between the elements of care planning that service users and practitioners found helpful and others that were required by the organization (meso state logics; Farr et al., 2019). Security restrictions (partly driven by precautionary approach to testing new electronic devices in the NHS–state logics) influenced staff’s ability to have a remote and live connection to the service user’s care information (Pithara et al., 2020). Integrating co-designed features (community logics) into the main electronic health record system (state logics) was also challenging.
Project End
Whilst the co-design process embraced a community logic at a micro level, ultimately cost (market and state) logics were dominant at the macro level that drove the decision-making as to whether to adopt the tool more widely, following the pilot. When the pilot was completed, financial pressures of the NHS organization meant the partnership between the Trust and software developers came to an end. Technological development in the NHS does not always show immediate impact, and ongoing challenges of IT interoperability, combined with the NHS struggling with resource and capacity issues, meant the organization was no longer able to invest in the CPT’s further development. The company co-designing the tool espoused a continuing commitment to prioritize working with service users and NHS staff to co-produce digital solutions aiming to enhance the delivery of mental healthcare.
Example 3—Youth Mental Health in Ontario, Canada
In Ontario, Canada, two concurrent provincial level public policy objectives were to improve transitions from child to adult mental health services and to enhance patient involvement in health service design more generally (Government of Ontario, 2006, 2011, 2015). Transitions to adult care were recognized to be a weak spot in health systems, with the child and adult health sectors governed by different ministries of government, and often adopting different care approaches, leaving youth vulnerable to falling through the cracks between systems (Randall et al., 2016). The design research was driven by an academic research team, who reached out at the meso level to organizations that collectively contributed to offering service prior to, during, and following transition to adult care.
Beginning of the Project
Over the years, a dominant profession logic was centered on a biomedical model of mental illness that had been contested by people with lived experience and family members who adopted a bio-psycho-social care logic to support mental health recovery (Mulvale & Bartram, 2015). Advocates for this community approach stressed that the involvement of people with lived experience and family members in designing mental health services would lead to improvements in a sector wherein clients’ voices had traditionally been repressed (Mulvale et al., 2007). This approach had garnered public policy support at the national and provincial levels, where previously a state and profession logic was more traditional (Government of Ontario, 2015; Mental Health Commission of Canada, 2012; Mulvale et al., 2014). Figure 6 shows how the Youth Mental Health Ontario project contributed to and was influenced by the evolution of logics using the Layers of Logics Map as a snapshot before and after the project.
While the rhetoric of a community approach was commonly voiced, operationalizing these concepts at the meso level for transitional aged youth (aged 16 to 25) moving between child and adult mental health services where contested logics were at play was challenging. At the meso level, child sector organizational mindsets featured a developmental bio-psycho-social care approach with significant family/caregiver involvement. In contrast, adult sector organizations, such as hospitals, were driven by a bio-medical orientation aimed at the median aged adult patient, and typically excluded family and caregivers, while regional health authorities held primarily market based logics aimed at efficiency of use of existing services (Mulvale et al., 2016). At the macro provincial government public policy level, state level bureaucratic logics entrenched differences in funding, payment, and regulations across child and adult sectors that served to entrench the contested sectoral logics.
Logic and Strategies through the Project
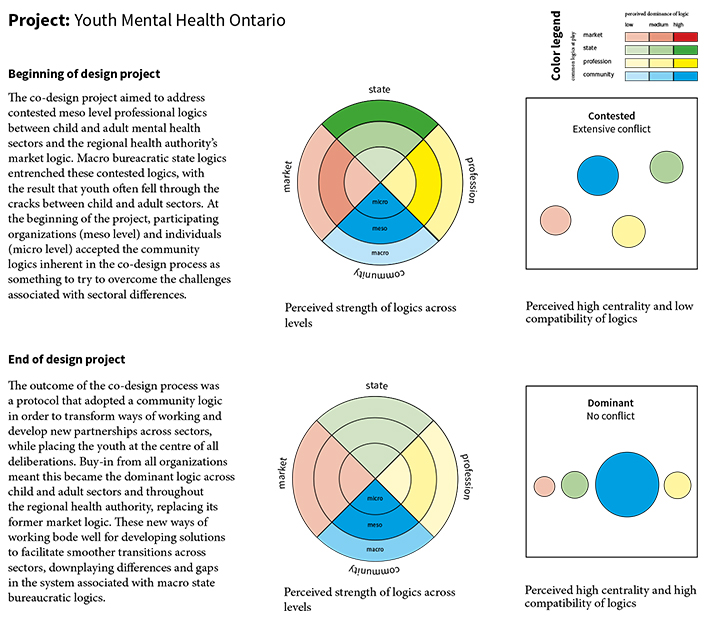
Figure 6. Youth Mental Health Ontario Layers of Logics Map.
The research design team adopted an experience-based co-design (EBCD) which is “an approach to improving healthcare services that combines participatory and user experience design tools and processes to bring about quality improvements in healthcare organisations” (Donetto et al., 2014, p. 11). EBCD applied a community logic that aimed to build mutual understanding and commitment from the major stakeholders at the micro level (youth, family/caregivers, and service providers) representing organizations that offer services prior to, during, or following transition to adult care. The objective of the research design team was to facilitate a process that began with focus groups by perspective where key touchpoints were identified, followed by a co-design event whereby mixed groups of participants would come to understand the system collaboratively and so plan and prototype improvements that aligned the various logics. At the micro level, youth and family/caregivers were fully aligned with the community logic and, although initially wary, service providers were open to engaging in the process. The research team augmented the traditional EBCD toolkit of identifying memorable service experience touchpoints, to surface the associated underlying values from each perspective as design principles to be adhered to during co-design activities. Each perspective thus felt honored and trusted that the process would respect their associated logics. The eventual solutions focused on prototypes of philosophical principles and new working relations rooted in a community logic, rather than concrete steps to improve transition experiences.
At End of Project
The EBCD processes were successful in aligning youth, family/caregivers, child service, and some adult provider mindsets toward a common community logic as the dominant logic going forward at the micro level. The open-ended approach to solutions received wide support at the meso level by enabling multiple organizations in child/youth and adult service delivery to locate themselves, and further aligned with the macro level state logic of enhancing patient engagement. Despite this success, sustaining adult sector providers’ involvement in the EBCD process was difficult, creating a risk that the professional logic might challenge implementation in some adult sector organizations at the meso levels, particularly in light of shifting public policy attention at the macro level. Despite initial end of project success, since completion of the co-design process, a changing policy context that reorganized governance within the health care system and the subsequent priority each organization had to place on pivoting to online care delivery during the pandemic has prohibited implementation to date. The limited action that has been taken suggests that the dominance of the community logic at the end of the co-design process can be fragile in the face of contextual changes that may result, in return, to pre-existing institutionalized and contested logics.
Discussion
The aim of this article is to surface potential logic conflicts and reflect on the implications for design, particularly within the context of public mental healthcare transformation. While previous literature has highlighted the potential of design to support a transformation of logics (Kurtmollaiev et al., 2018); stressed the need for designers’ reflexivity (Sangiorgi, 2011); and called for the acknowledgement of existing logics when working to catalyze transformational change (Junginger, 2015), there has not been a lot of practical support regarding how this can be done. To aid in making the multiplicity of logics more explicit, within both a particular context and a specific design project, we developed the Layers of Logics Map. This map can help designers and researchers reflect on the plurality of logics at play across levels of aggregation and aid in anticipating future logic conflicts. In the context of public mental healthcare, we identified four predominant logics that were necessary to reflect on: the logic of the state; the logic of the market; the logic of professions; and the logic of the community. While the map is not fixed to these particular archetypical logics and can be adapted to reflect the logics in different contexts, this version of the map helped us to unpack and explore the patterns of designing with and within different, sometimes conflicting logics, as they related to co-design and co-production in mental healthcare. Through the examples discussed, it becomes clear that not all logics are explicit and visible, and may be invisible or assumed at different stages of a project, only surfacing through actions and decisions through time. The co-design process, including its methods and approaches, can aid in making these hidden logics more explicit by leveraging their affordances for different modes of reflexivity (Vink & Koskela-Huotari, 2021a).
The different project stories presented above show how designers or design-based approaches, such as EBCD, can encounter different logics when aiming to introduce more collaborative approaches in mental healthcare. These design approaches seem to influence logics of project stakeholders at the micro and meso levels of aggregation, but also have to engage with the impact and influence of macro level pressures. In all three examples, design acts in apparent alignment with a policy goal or shared ambition at the macro level that can embody varying degrees of a state or market logic and that legitimates actions that have direct influence at the micro and then meso levels. In practice, this alignment might continue down to the meso and micro level—as in the first example—creating pragmatic agreements across conflicting logics, generating legitimacy of a design approach adopting or translating design inputs into other logics’ language (e.g., evidence-based), or establishing a dominant logic at the micro level to find a way to converge and implement an effective solution. In other cases, this alignment might be lost, when co-design processes introduce a more community logic that might not align with logics at the meso and macro levels. For example, whilst there can be visible collaboration and aligned logics at a micro level during the design and pilot implementation process, when wider organizational decisions have to be made about further implementation more contradictory logics can surface (example 2). These misalignments can be temporarily overcome in the duration of the design process via generating more open-ended approaches (example 3), but when the discourse goes back to a macro level and fundamental decision-making stages, different dominant logics or unsolved conflicts might become more evident again, or the policy agenda might need to change the direction and priorities.
These examples show the important role of collective alignment in realizing long-term change in service ecosystems with a multiplicity of logics (Vink et al., 2021b). With regards to the transformation of mental healthcare, they also exemplify how co-design and co-production can take on or promote a variety of logics, in many cases upholding rather than disrupting existing power dynamics (Farr, 2019). While reflection on these dynamics can help to build awareness and intentionality within the design process, it is important to note that logics are often highly institutionalized and taken for granted, making them difficult to become aware of (Greenwood et al., 2008).
While the Logic Multiplicity Workbook and Layers of Logics Map can help to make them more explicit, the full visibility of these logics and their conflicts may never be fully understood. The map can in fact support design teams to discuss and reflect only on the perceived strengths of multiple logics at play at different levels of the ecosystem, and to consider the impact of their interaction in terms of the perceived centrality and compatibility of logics at different moments of a design process. Taking frequent project logic snapshots over the course of a project can increase the reflexivity of design teams on the consequences of adopted strategies or the need for new ones to try to reduce conflicts toward a more balanced coexistence, to align with more dominant logics, to ignite contestation, or to consider temporary estrangement.
Limitations
This article is subject to limitations in terms of who was involved in this retrospective analysis and the level of data available, which certainly influenced perceptions of the results of the Workbook and Layers of Logics Map as tools. Furthermore, in order for these tools to be accessible for use, they were somewhat simplified, and there is recognition that many of the logics were entangled, difficult to separate, and sometimes their levels of influence and the levels of resulting conflict were challenging to differentiate. As a result, the Workbook and Layers of Logics Map are just tools among many approaches that should be employed to support reflection and learning before, during, and after a design process.
It is also important to recognize that this research builds on an understanding of common logics within Western society in the context of North American and European mental health systems. As such, further research is needed to understand the logics in non-Western societies and how they might relate to designing for co-production (or an alternative goal) in relation to mental health. In addition, while we focus on the public mental health context, there is a need to explore how the Layers of Logics Map could be adapted to support reflection on the multiplicity of logics in other settings.
While this research unpacks project examples retrospectively, future practice and research could explore the benefits and challenges of using the Logic Multiplicity Workbook and the Layers of Logics Map prior to or during a design process to inform ongoing design efforts and catalyze conversations about the goals and how to work with and within existing logics. This could happen by integrating the Workbook and the Map into a co-design process, developing them further to become more structured participatory tools (similar to a design game) and approaches, with integrated tips, examples, and collaboration strategies. They could then be applied at certain stages of designing to enhance the capability of participants to fully grasp the concept of logics, better recognize their dynamics and manifestations, and inform decision making.
Conclusions
Navigating within and across logic multiplicity is a skill that designers increasingly need to hone as they work in complex service ecosystems with a variety of legacy systems and new entrants in place. The Logic Multiplicity Workbook and the Layers of Logics Map offer support for researchers and design team members for considering the multiple logics at play that manifest at different levels and points in time, which might not otherwise be fully evident or part of the ongoing strategic discussion. Becoming more mindful of designers’ and other participants’ roles in enacting or undermining logics is increasingly critical within design. Our hope is that this work, exploring the multiplicity of logics when co-designing services in public mental healthcare, inspires others to do the same within their own settings, and that together we continue to build up the supports to enhance reflexivity when designing amid complexity.
Acknowledgments
The Example 2–Care Pathway Tool research was supported by the National Institute for Health Research (NIHR) Applied Research Collaboration West (NIHR ARC West). The views expressed in this article are those of the authors and not necessarily those of the NIHR or the Department of Health and Social Care.
References
- Akama, Y., & Yee, J. (2019). Special issue: Embracing plurality in designing social innovation practices. Design and Culture, 11(1), 1-11. https://doi.org/10.1080/17547075.2019.1571303
- Arman, R., Liff, R., & Wikström, E. (2014). The hierarchization of competing logics in psychiatric care in Sweden. Scandinavian Journal of Management, 30(3), 282-291. https://doi.org/10.1016/j.scaman.2014.01.001
- Bailey, S. (2012). Embedding service design: The long and the short of it. In Proceedings of the 3rd Nordic conference on service design and service innovation (pp. 1-11). Laurea University of Applied Sciences.
- Bason, C. (2010). Leading public sector innovation: Co-creating for a better society. The Policy Press.
- Bee, P., Brooks, H., Fraser, C., & Lovell, K. (2015). Professional perspectives on service user and carer involvement in mental health care planning: A qualitative study. International Journal of Nursing Studies, 52(12), 1834-1845. https://doi.org/10.1016/j.ijnurstu.2015.07.008
- Beresford, P. (2016). From psycho-politics to mad studies: Learning from the legacy of Peter Sedgwick. Critical and Radical Social Work, 4(3), 343-55. https://doi.org/10.1332/204986016X14651166264237
- Besharov, M. L., & Smith, W. K. (2014). Multiple institutional logics in organizations: Explaining their varied nature and implications. Academy of Management Review, 39(3), 364-381. https://doi.org/10.5465/amr.2011.0431
- Borgers, P., & Tomlinson, K. (2017). Crazywise film. Retrieved October 25, 2020, from https://crazywisefilm.com/
- Brooks, H. L., Lovell, K., Bee, P., Sanders, C., & Rogers, A. (2018). Is it time to abandon care planning in mental health services? A qualitative study exploring the views of professionals, service users and carers. Health Expectations, 21(3), 597-605. https://doi.org/10.1111/hex.12650
- Capano, G. (2019). Reconceptualizing layering–From mode of institutional change to mode of institutional design: Types and outputs. Public Administration, 97(3), 590-604. https://doi.org/10.1111/padm.12583
- Cloutier, C., & Langley, A. (2013). The logic of institutional logics: Insights from French pragmatist sociology. Journal of Management Inquiry, 22(4), 360-380. https://doi.org/10.1177/1056492612469057
- Crossley, N. (1998). R. D. Laing and the British anti-psychiatry movement: A socio–historical analysis. Social Science & Medicine, 47(7), 877-889. https://doi.org/10.1016/S0277-9536(98)00147-6
- Currie, W. L., & Guah, M. W. (2007). Conflicting institutional logics: A national programme for IT in the organisational field of healthcare. Journal of Information Technology, 22(3), 235-247. https://doi.org/10.1057/palgrave.jit.2000102
- Department of Health. (2008). Refocusing the care programme approach: Policy and positive practice guidance. Department of Health, Great Britain. https://webarchive.nationalarchives.gov.uk/ukgwa/20130107105354/http:/www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/@dh/@en/documents/digitalasset/dh_083649.pdf
- De Zulueta, P. (2013) Compassion in 21st century medicine: Is it sustainable? Clinical Ethics. 8(4), 119-128. https://doi.org/10.1177/1477750913502623
- Donetto, S., Tsianakas, V., & Robert, G. (2014). Using Experience-based Co-design (EBCD) to improve the quality of healthcare: mapping where we are now and establishing future directions. King’s College London.
- Dubois, A., & Gadde, L. E. (2002). Systematic combining: An abductive approach to case research. Journal of Business Research, 55(7), 553-560. https://doi.org/10.1016/S0148-2963(00)00195-8
- Dunleavy, P., & Hood, C. (1994). From old public administration to new public management. Public Money & Management, 14(3), 9-16. https://doi.org/10.1080/09540969409387823
- Dunn, M. B., & Jones, C. (2010). Institutional logics and institutional pluralism: The contestation of care and science logics in medical education, 1967-2005. Administrative Science Quarterly, 55, 114-149. https://doi.org/10.2189/asqu.2010.55.1.114
- Escobar, A. (2018). Designs for the Pluriverse. Duke University Press.
- Farr, M. (2013). Citizens and the co-creation of public service innovations. In S. P. Osborne & L. Brown (Eds.), Handbook of innovation in public services (pp. 152-172). Edward Elgar.
- Farr, M. (2019). Co-design and co-production in public services: A governance analysis approach. In E. Carmel (Ed.), Governance analysis: Critical enquiry at the intersection of politics, policy and society (pp. 623-644). Edward Elgar. https://doi.org/10.1530/EJE-14-0355
- Farr, M., Pithara, C., Sullivan, S., Edwards, H., Hall, W., Gadd, C., Walker, J., Hebden, N., & Horwood, J. (2019). Pilot implementation of co-designed software for co-production in mental health care planning: A qualitative evaluation of staff perspectives. Journal of Mental Health, 28(5), 495-504. https://doi.org/10.1080/09638237.2019.1608925
- Fligstein, N., & McAdam, D. (2012). A theory of fields. Oxford University Press.
- Friedland, R., & Alford, R. (1991). Bringing society back in: Symbols, practices, and institutional contradictions. In W. Powell & P. DiMaggio (Eds.), The new institutionalism in organizational analysis (pp. 232-263). University of Chicago Press.
- Friedland, R. (2013). The value of institutional logics. In G. Kruecken, C. Mazza, R. Meyer, & P. Walgenbach (Eds.), New themes in institutional analysis (pp. 12-50). Edward Elgar. https://doi.org/10.4337/9781784716875.00006
- Garety, P. (2001). Making sense of voices. Psychiatric Bulletin, 25(10), 406-407. https://doi.org/10.1192/pb.25.10.406-a
- Goodrick, E., & Reay, T. (2011). Constellations of institutional logics: Changes in the professional work of pharmacists. Work and Occupations, 38(3), 372-416. https://doi.org/10.1177/0730888411406824
- Gopalkrishnan, N., & Babacan, H. (2015). Cultural diversity and mental health. Australasian Psychiatry, 23(6), 6-8. https://doi.org/10.1177/1039856215609769
- Government of Ontario. (2015). Patients first: Action plan for health care. Retrieved from http://www.health.gov.on.ca/en/ms/ecfa/healthy_change/docs/rep_patientsfirst.pdf
- Government of Ontario. (2011). Open minds, healthy minds: Ontario’s comprehensive mental health and addictions strategy. Retrieved from http://www.health.gov.on.ca/en/common/ministry/publications/reports/mental_health2011/mentalhealth_rep2011.pdf
- Government of Ontario. (2006). A shared responsibility: Ontario’s policy framework for child and youth mental health. Retrieved from http://www.children.gov.on.ca/htdocs/English/documents/specialneeds/mentalhealth/framework.pdf
- Greenwood, R., Oliver, C., Sahlin, K., & R. Suddaby (2008). Introduction. In R. Greenwood, C. Oliver, K. Sahlin, & R. Suddaby (Eds.), SAGE Handbook of Organizational Institutionalism (pp. 1-46). SAGE.
- Greenwood, R., Raynard, M., Kodeih, F., Micelotta, E. R., & Lounsbury, M. (2011). Institutional complexity and organizational responses. Academy of Management Annals, 5(1), 317-371. https://doi.org/10.1080/19416520.2011.590299
- Greenwood, R., Oliver, C., Lawrence, T. B., & Meyer, R. E. (Eds.) (2017). The Sage handbook of organizational institutionalism (2nd ed). SAGE.
- Grenha Teixeira, J., Patrício, L., Huang, K-H., Fisk, R. P., No ́brega, L., & Constantine, L. (2017). The minds method: Integrating management and interaction design perspectives for service design. Journal of Service Research, 20(3), 240-258. https://doi.org/10.1177/1094670516680033
- Holmlid, S. (2009). Participative, co-operative, emancipatory: From participatory design to service design. In Proceedings of the 1st Nordic conference on service design and service innovation (pp. 1-14). Linköping University Electronic Press.
- Hussain, S., Sanders, E. B. N., & Steinert, M. (2012). Participatory design with marginalized people in developing countries: Challenges and opportunities experienced in a field study in Cambodia. International Journal of Design, 6(2), 91-109.
- Jaakkola, E., Aarikka-Stenroos, L., & Ritala, P. (2019). Institutionalization process of service innovation: Overcoming competing institutional logics in service ecosystems. In P. P. Maglio, C. A. Kieliszewski, J. C. Spohrer, K. Lyons, Y. Sawatani, & L. Patrício (Eds.), Handbook of service science (Vol. 2, pp. 497-516). Springer.
- Julier, G. (2006). From visual culture to design culture. Design Issues, 22(1), 64-76. https://doi.org/10.1162/074793606775247817
- Johnstone, L., & Boyle, M. (2018). The power threat meaning framework. British Psychological Society. https://www.bps.org.uk/sites/bps.org.uk/files/Policy%20-%20Files/PTM%20Main.pdf
- Joly, M. P., Teixeira, J. G., Patrício, L., & Sangiorgi, D. (2019). Leveraging service design as a multidisciplinary approach to service innovation. Journal of Service Management, 30(6) 681-715. https://doi.org/10.1108/JOSM-07-2017-0178
- Junginger, S. (2015). Organizational design legacies and service design. Design Journal, 18(2), 209-226. https://doi.org/10.2752/175630615X14212498964277
- Junginger, S., & Sangiorgi, D. (2009). Service design and organisational change: Bridging the gap between rigour and relevance. In Proceedings of the 3rd IASDR conference on design research (pp. 4339-4348). Korean Society of Design Science.
- Kelly, G., Mulgan, G., & Muers, S. (2002). Creating public value: An analytical framework for public service reform. United Kingdom Cabinet Office.
- Kensing, F., & Blomberg, J. (1998). Participatory design: Issues and concerns. Computer Supported Cooperative Work, 7, 167-185. http://doi.org/10.1023/A:1008689307411
- Kimbell, L., & Bailey, J. (2017). Prototyping and the new spirit of policy-making. CoDesign, 13(3), 214-226. https://doi.org/10.1080/15710882.2017.1355003
- Kurtmollaiev, S., Fjuk, A., Pedersen, P., Clatworthy, S., & Kvale, K. (2018) Organizational transformation through service design: The institutional logics perspective. Journal of Service Research, 21(1), 59-74. https://doi.org/10.1177/1094670517738371
- McMullin, C. (2020). Co-production of public services: Institutional barriers to the involvement of citizens in policy implementation. In H. Sullivan, H. Dickinson, & H. Henderson (Eds.), The palgrave handbook of the public servant (pp. 1-17). Springer. https://doi.org/10.1007/978-3-030-03008-7_26-1
- Meyer, J., & Rowan, B. (1977). Institutionalized organizations: Formal structure as myth and ceremony. American Journal of Sociology, 83(2), 340-363. http://www.jstor.org/stable/2778293
- Mental Health Commission of Canada. (2012). Changing directions changing lives: The mental health strategy for Canada. Retrieved from https://www.mentalhealthcommission.ca/wp-content/uploads/drupal/MHStrategy_Strategy_ENG.pdf
- Mental Health Taskforce. (2016). Five year forward view for mental health. NHS England. https://www.england.nhs.uk/mentalhealth/taskforce/
- Mol, A. (2008). The logic of care. Routledge.
- Mulvale, G., Nguyen, T., Miatello, A., Embrett, M., Wakefield P., & Randall, G. E. (2016). Lost in transition or translation? Care philosophies and transitions between child and youth and adult mental health services: A systematic review. Journal of Mental Health, 28(4), 379-388. https://doi.org/10.3109/09638237.2015.1124389
- Mulvale, G., & Bartram, M. (2015). No more ‘us’ and ‘them’: Integrating recovery and well-being into a conceptual model for mental health policy. Canadian Journal of Community Mental Health, 34(4), 31-67. https://doi.org/10.7870/cjcmh-2015-010
- Mulvale, G., Chodos, H., Bartram, M., MacKinnon, M. P., & Abud, M. (2014). Engaging civil society through deliberative dialogue to create the first mental health strategy for Canada: Changing directions, changing lives. Social Science and Medicine, 123, 262-268. https://doi.org/10.1016/j.socscimed.2014.07.029
- Mulvale, G., Abelson, J., & Goering, P. (2007). Mental health service delivery in Ontario Canada: How do policy legacies shape prospects for reform? Health Economics, Policy and Law, 2(4), 363-389. https://doi.org/10.1017/S1744133107004318
- Osborne, S. P. (2010). The new public governance? Emerging perspectives on the theory and practice of public governance. Routledge.
- Osborne, S. P. (2018). From public service-dominant logic to public service logic: Are public service organizations capable of co-production and value co-creation? Public Management Review, 20(2), 225-231. https://doi.org/10.1080/14719037.2017.1350461
- Pestoff, V. (2018). Co-production at the crossroads of public administration regimes. In T. Brandsen, T. Steen, & B. Verschuere (Eds.), Co-production and co-creation: Engaging citizens in public services (pp. 27-36). Routledge. https://doi.org/10.4324/9781315204956
- Pierri, P., Warwick, L., & Garber, J. (2016). Embedding design in a mental health network. In Proceedings of the service design geographies (pp. 580-585). Linköping University Electronic Press.
- Pithara, C., Farr, M., Sullivan, S., Edwards, H., Hall, W., Gadd, C., Walker, J., Hebden, N., & Horwood, J. (2020). Implementing a digital tool to support shared care planning in community-based mental health services: Qualitative evaluation. Journal of Medical Internet Research, 22(3), e14868. https://doi.org/10.2196/14868
- Prahalad, C. K., & Bettis, R. (1986). The dominant logic: A new linkage between diversity and performance. Strategic Management Journal, 7(6), 485-501. https://www.jstor.org/stable/2486135
- Provan, K. G., Isett, K. R., & Milward, H. B. (2004). Cooperation and compromise a network response to conflicting institutional pressures in community mental health. Non Profit and Voluntary Sector Quarterly, 33(3), 489-514. https://doi.org/10.1177/0899764004265718
- Rainford, P., & Tinkler, J. (2011). Designing digital public services. Retrieved from http://eprints.lse.ac.uk/37812/1/Designing_digital_public_services_%28lsero%29.pdf
- Randall, G. E., Mulvale, G. M., Wakefield, P. A., Embrett, M. G., Barr, N. G., Miatello, A. M., Longo, C. J., Nguyen, T. D., Di Rezze, B. M., Vania, D. K., & McRae, S. A. (2016). Mapping the policy to practice landscape for youth mental health in Ontario: A report from the “youth to adult transitions in health care – The case of mental health services in Ontario” research team. McMaster University.
- Reay, T., & Hinings, C. R. (2009). Managing the rivalry of competing institutional logics. Organization Studies, 30(6), 629-652. https://doi.org/10.1177/0170840609104803
- Reay, T., Goodrick, E., Waldorff, S. B., & Casebeer, A. (2017). Getting leopards to change their spots: Co-creating a new professional role identity. Academy of Management Journal, 60(3), 1043-1070. https://doi.org/10.5465/amj.2014.0802
- Rose, D., & Kalathil, J. (2019). Power, privilege and knowledge: The untenable promise of co-production in mental ‘health’. Frontiers in Sociology, 4, 1-11. https://doi.org/10.3389/fsoc.2019.00057
- Sangiorgi, D. (2011). Transformative services and transformation design. International Journal of Design, 5(2), 29-40.
- Sangiorgi, D., Farr, M., McAllister, S., Mulvale, G., Sneyd, M., Vink, J. E., & Warwick, L. (2019). Designing in highly contentious areas: Perspectives on a way forward for mental healthcare transformation. The Design Journal, 22(sup1), 309-330. https://doi.org/10.1080/14606925.2019.1595422
- Sangiorgi, D., Patrício, L., & Fisk, R. (2018). Designing for interdependence, participation and emergence in complex service systems. In D. Sangiorgi & A. Prendiville (Eds.), Designing for service: Key issues and new directions (pp. 49-64). Bloomsbury. https://doi.org/10.5040/9781474250160.ch-004
- Sanders, E. B. N., & Stappers, P. J. (2008). Co-creation and the new landscapes of design. CoDesign, 4(1), 5-18. https://doi.org/10.1080/15710880701875068
- Scheid, T. L. (2000). Rethinking professional prerogative: Managed mental health care. Sociology of Health & Illness, 22(5), 700-719. https://doi.org/10.1111/1467-9566.00227
- Scheid, T. L. (2003). Managed care and the rationalization of mental health services. Journal of Health and Social Behavior, 44(2), 142-161. https://doi.org/10.2307/1519805
- Scheid, T. (2008). Competing institutional demands: A framework for understanding mental health policy. Social Theory Health, 6(4), 291-308. https://doi.org/10.1057/sth.2008.12
- Schultz, T., Abdulla, D., Ansari, A., Canli, E., Keshavarz, M., Kiem, M., de O. Martins, L. P., & Oliveira, P. (2018). What is at stake with decolonizing design? A roundtable. Design and Culture, 10(1), 81-101. https://doi.org/10.1080/17547075.2018.1434368
- Scott, W. R., Ruef, M., Mendel, P. J., & Caronna, C. A. (2000). Institutional change and healthcare organizations: From professional dominance to managed care. University of Chicago Press
- Shostack, G. L. (1984). Designing services that deliver. Harvard Business Review, 62(1), 133-139.
- Siltaloppi, J., Koskela-Huotari, K., & Vargo, S. L. (2016). Institutional complexity as a driver for innovation in service ecosystems. Service Science, 8(3), 333-343. https://doi.org/10.1287/serv.2016.0151
- Spitzmueller, M. C. (2018). Remaking “community” mental health: Contested institutional logics and organizational change. Human Service Organizations Management, Leadership and Governance, 42(2), 123-145. https://doi.org/10.1080/23303131.2017.1422071
- Tan, L. (2012). Understanding the different roles of the designer in design for social good: A study of design methodology in the DOTT 07 (Designs of the Times 2007) projects [Doctoral dissertation]. Northumbria University.
- Taffe, S. (2015). The hybrid designer/end-user: Revealing paradoxes in co-design. Design Studies, 40, 39-59. https://doi.org/10.1016/j.destud.2015.06.003
- Thornton, P., Ocasio, W., & Lousbury, M. (2012). The institutional logic perspective: A new approach to culture, structure, and process. Oxford University Press.
- Thornton, P., & Ocasio, W. (1999). Institutional logics and the historical contingency of power in organizations: Executive succession in the higher education publishing industry, 1958-1990. American Journal of Sociology, 105(3), 801-843. https://doi.org/10.1086/210361
- Trischler, J., Pervan, S. J., Kelly, S. J., & Scott, D. R. (2018). The value of codesign: The effect of customer involvement in service design teams. Journal of Service Research, 21(1), 75–100. https://doi.org/10.1177/1094670517714060
- Tlostanova, M. (2017). On decolonizing design. Design Philosophy Papers, 15(1), 51-61. https://doi.org/10.1080/14487136.2017.1301017
- Tõnurist, P., Kattel, R., & Lember, V. (2017). Innovation labs in the public sector: What they are and what they do? Public Management Review, 19(10), 1455-1479. https://doi.org/10.1080/14719037.2017.1287939
- Vickers, I., Lyon, F., Sepulveda, L., & McMullin, C. (2017). Public service innovation and multiple institutional logics: The case of hybrid social enterprise providers of health and wellbeing. Research Policy, 46(10), 1755-1768. https://doi.org/10.1016/j.respol.2017.08.003
- Vink, J., & Koskela-Huotari, K. (2021a). Building reflexivity using service design methods. Journal of Service Research. https://doi.org/10.1177/10946705211035004
- Vink, J., Koskela-Huotari, K., Tronvoll, B., Edvardsson, B., & Wetter-Edman, K. (2021b). Service ecosystem design: Propositions, process model, and future research agenda. Journal of Service Research, 24(2) 168-186. https://doi.org/10.1177/1094670520952537
- Vink, J., Edvardsson, B., Wetter-Edman, K., & Tronvoll, B. (2019). Reshaping mental models: Enabling innovation through service design. Journal of Service Management, 30(1), 75-104. https://doi.org/10.1108/JOSM-08-2017-0186
- Vink, J., Wetter-Edman, K., & Rodrigues, V. (2017). Designing good(s)? Exploring the politics of social design processes. In Proceedings of the design management academy conference (pp. 961-977). Digitala Vetenskapliga Arkivet. https://doi.org/10.21606/dma.2017.131
- Visser, F. S., Stappers, P. J., van der Lugt, R., & Sanders, E.B.-N. (2005). Contextmapping: Experiences from practice. CoDesign, 1(2), 119-149. https://doi.org/10.1080/15710880500135987
- Waldorff, S., Reay, T., & Goodrick, E. (2013). A tale of two countries: How different constellations of logics impact action. In M. Lounsbury & E. Boxenbaum (Eds.), Institutional logics in action, Vol: 39, Part A. Research in the sociology of organizations (pp. 99-129). Emerald Group Publishing.
- Warwick, L., Tinning, A., Smith, N., & Young, R. (2018). Co-designing wellbeing: The commonality of needs between co-designers and mental health service users. In Proceedings of the DRS international conference (pp. 25-28). Design Research Society. https://doi.org/10.21606/drs.2018.405
- Warwick, L. (2015). Can design effect transformational change in the voluntary community Sector? [Doctoral dissertation]. Northumbria University.
- Wetter-Edman, K. (2012). Relations and rationales of user’s involvement in service design and service management. In S. Miettinen & A. Valtonen (Eds.), Service design with theory: Discussions on change, value and methods (pp. 107-116). Lapland University Press.
- Wetter-Edman, K., Vink, J., & Blomkvist, J. (2018). Staging aesthetic disruption through design methods for service innovation. Design Studies, 55, 5-26. https://doi.org/10.1016/j.destud.2017.11.007
- Willis, A. M. (2018). Design philosophy reader. Bloomberg.
- Yu, E., & Sangiorgi, D. (2018). Service design as an approach to implement the value cocreation perspective in new service development. Journal of Service Research, 21(1), 40-58.
- Zomerdijk, L., & Voss, C. (2010). NSD processes and practices in experiential services. Journal of Product Innovation Management, 28(1), 63-80. https://doi.org/10.1111/j.1540-5885.2010.00781.x
Appendix
Examples of Logic Multiplicity Workbook applied to the Care Pathway Tool and Youth Mental Health Ontario case studies, applied at two moments of the project: at the beginning T1 and at the end of the project T2. To find the original excel version of the tool, please visit http://www.ijdesign.org/materials/4171_Appendix_LogicMultiplicityWorkbook_Tool.xlsx

Appendix 1. Care Pathway Tool case study analyzed at the beginning of the project (T1).

Appendix 2. Care Pathway Tool case study analyzed at the end of the project (T2).
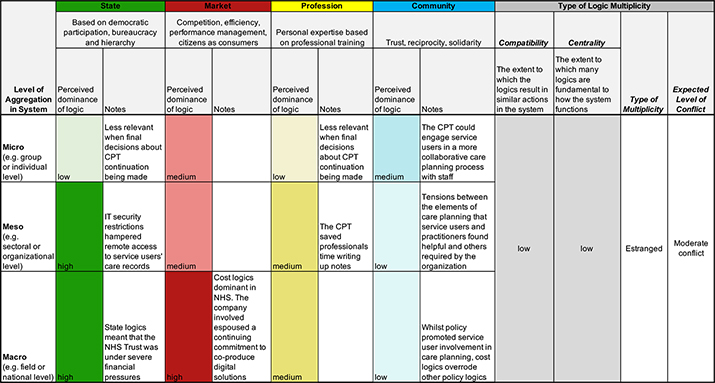
Appendix 3. Youth Mental Health Ontario analyzed at the beginning of the project (T1).
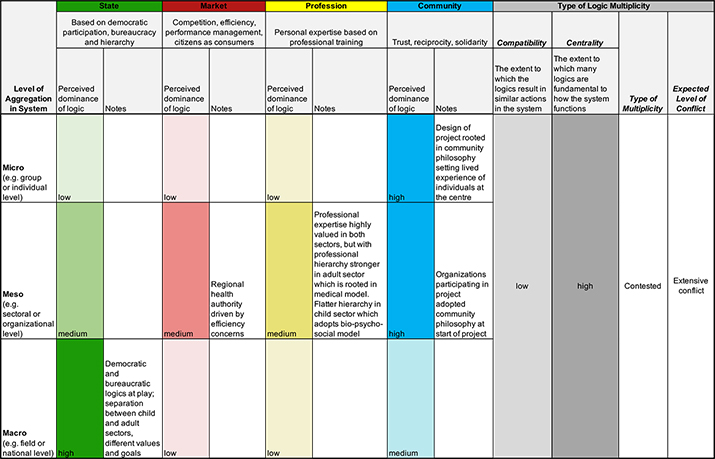
Appendix 4. Youth Mental Health Ontario analyzed at the end of the project (T2).