
Kitchen Living in Later Life: Exploring Ergonomic Problems, Coping Strategies and Design Solutions
Martin Maguire 1,*, Sheila Peace 2, Colette Nicolle 1, Russell Marshall 1, Ruth Sims 1, John Percival 2, and Clare Lawton 1
Loughborough Design School, Loughborough University, Loughborough, UK
Faculty of Health and Social Care, The Open University, Milton Keynes, UK
The kitchen is an important area in the home serving many purposes both functional and social. It is central to enabling people to stay within their own homes in their later life. As part of a detailed study of ‘past’ and ‘present’ kitchen living, semi-structured interviews were conducted with 48 older people about their current kitchen and how well it met their needs. It was found that personal problems with reaching, bending, dexterity and sight were more likely to be experienced with increasing age while for specific tasks, ironing and cleaning created the most difficulty. The paper reports on coping strategies and simple innovations made by the participants to address the problems they experienced. A challenge for kitchen designers, manufacturers and installers is to think in terms of kitchens that are more flexible and adaptable to people’s changing needs.
Keywords – Kitchen Design, Kitchen Ergonomics, Inclusive Design, Older People.
Relevance to Design Practice – The research identifies problems that older people experience in the kitchen and any coping strategies or design solutions employed. This is intended to inspire more inclusive kitchen design, promote independent living in later life, and recognise the value of lifetime homes.
Citation: Maguire, M., Peace, S., Nicolle, C., Marshall, R., Sims, R., Percival, J., & Lawton, C. (2014). Kitchen living in later life: Exploring ergonomic problems, coping strategies and design solutions. International Journal of Design, 8(1), 73-91.
Received May 14, 2012; Accepted July 5, 2013; Published April 30, 2014.
Copyright: © 2014 Maguire, Peace, Nicolle, Marshall, Sims, Percival, and Lawton. Copyright for this article is retained by the authors, with first publication rights granted to the International Journal of Design. All journal content, except where otherwise noted, is licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 2.5 License. By virtue of their appearance in this open-access journal, articles are free to use, with proper attribution, in educational and other non-commercial settings.
*Corresponding Author: m.c.maguire@lboro.ac.uk
Martin Maguire obtained his Master’s degree in Ergonomics from Loughborough University and was awarded a PhD in Human-Computer Interaction at Leicester Polytechnic before becoming a research associate in the Graphics Laboratory at Leicester University. Since then he has worked at Loughborough University as a human factors researcher and practitioner for the Human Sciences and Advanced Technology (HUSAT) Research Institute and the Ergonomics and Safety Research Institute (ESRI). He is now a Research Fellow and Lecturer in the Loughborough Design School. Martin has been involved in many research and consultancy projects including the design of software, equipment and environments to be usable, engaging and inclusive for all people particularly novice users. He has also worked on a number of European Commission projects to develop tools for usability design and UK Research Council projects on designing for older people in different contexts, including the kitchen.
Sheila Peace is Professor of Social Gerontology in the Faculty of Health and Social Care at The Open University. She is an Academician of the Social Sciences and a long term member of the British Society of Gerontology currently President Elect, a post that she will take up in 2014. A social geographer by first discipline, Sheila has a PhD centred in Environmental Gerontology from the University of Swansea. She specialises in research concerning ageing in context spanning 35 years and relating to both macro and micro environmental settings including: quality of life and the design of care homes; regulation of care homes; living in mainstream and supportive housing in later life and impact on identity; intergenerational social interaction in public spaces; the creation of age-friendly cities/communities; the value of public/private space/place, and the views of older people on domestic design. Most recently work concerning the kitchen in later life with Loughborough University Design School which has seen the collaboration between gerontology, ergonomics and design.
Colette Nicolle started her career in human factors at the Human Sciences and Advanced Technology (HUSAT) Research Institute, then worked for the Ergonomics and Safety Research Institute (ESRI), and is now a Senior Lecturer and Research Fellow at the Loughborough Design School, Loughborough University. She is a Fellow of the Ergonomics Society, member of ANEC’s Design for All Working Group and their representative on CEN TC 122 ‘Ergonomics’. Her applied research and teaching focuses on inclusive design, ageing and disability in a range of application areas. This includes the development and promotion of user-centred and inclusive design methods and tools; the design and evaluation of inclusive products, technologies, and services; mobility and inclusion of older and disabled travellers; and the social and ethical implications of new technologies in particular for older users. Colette led Loughborough’s research on the EPSRC i~design3 project, and was a co-investigator for the New Dynamics of Ageing projects Working Late and Transitions in Kitchen Living.
Russell Marshall is a Senior Lecturer and Head of the Design Ergonomics Group in the Design School at Loughborough University. He received a MEng in Product Design and Manufacturing Engineering, and was awarded a PhD in Modular Product Design. His research interests cover a broad range of topics within product, industrial and engineering design including: digital human modelling and tools and techniques for facilitating and empowering designers in human-centred and inclusive design practice, ergonomics and human factors in design, modular product design, and drawing and visualisation. Russell is also principal developer of SAMMIE the digital human modelling system.
Ruth Sims studied Psychology at the University of Exeter, and completed an MSc in Ergonomics at Loughborough University before becoming a research associate at the same institution and completing her PhD in the area of ‘inclusive design/design for all. At Loughborough, Ruth worked on a variety of research projects, predominantly focused on issues regarding accessibility and usability of products, services and environments by older and physically impaired individuals. Ruth is now Senior Lecturer at the University of Derby where she teaches both online and on-campus, on the MSc Ergonomics courses and BSc Psychology courses, as well as continuing her research career.
John Percival is a researcher, social worker and independent consultant. He has been involved in health and social care research studies with University College London, Open University, University of Bath and University of Bristol. His mainly qualitative research work has focused on: older people’s housing needs and preferences; the impact of sight loss on social exclusion; lay and professional perspectives on telecare service development; assistive technology and its home uses for people with disabilities; and the quality of end-of-life care services, in nursing and residential homes, as well as in mainstream housing. John has recently edited a book on return migration in later life and its public policy implications. John’s key research interests include: the relationship between housing, support and social care needs; the emotional, psychological and practical implications of sight loss; technology and health monitoring in the homes of frail and vulnerable people; and qualitative research as a policy and practice tool.
Clare Lawton is a researcher at Loughborough University’s Design School. Over the last 10 years she has specialised in workplace and vehicle ergonomics. Prior to this Clare worked as an ergonomist at the Health and Safety Laboratory. She has a BSc in Cognitive Science from Sheffield University and a Master’s degree in Ergonomics from Loughborough University. Clare was awarded the Ergonomics Society Bursary of 1999 and the Stephen Pheasant Memorial Award in 2000 for her work regarding musculoskeletal disorders. She is currently working, as a human factors researcher on a five year research project i-STUTE the Interdisciplinary Centre for Storage, Transformation and Upgrading of Thermal Energy funded through the UK Research Councils’ Energy Programme. The project will develop technologies to reduce energy consumption and deliver cost-effective heating and cooling which will help the UK achieve its target of a reduction in greenhouse gas emissions of 80% by 2050.
Introduction
The kitchen environment needs to be both comfortable and usable if it is to support independent living for older people. The Transitions in Kitchen Living (TiKL) study presented here, was a project within the UK Research Council’s New Dynamics of Ageing programme (2006-2013). The aim of this research was to develop a holistic approach to understanding person-environment fit (Peace, Wahl, Mollenkopf, & Oswald, 2007) leading to informed design practice. In bringing together ergonomists and social gerontologists, it began by recording memories of kitchen life as an important record of social history and then to investigate people’s experiences of their current kitchen, whether it suited their capabilities and needs or required them to adopt coping strategies. This paper reports on the contemporary kitchen experience from an ergonomics perspective and identifies the problems faced and strategies adopted. A central aim of the study was to produce guidance for older people to help them perform kitchen tasks more easily and make adaptations to the kitchen to match their evolving needs.
The TiKL research builds on earlier studies. Design recommendations for comfort and safety in the kitchen design are offered by Moore and Ostrander (1992), Câmera (2010), Lin (2008), Huppert (2003) and Odén, Beck-Friis, & Östlund (2010). Guidance concerning domestic lighting was provided through the Thomas Pocklington Trust (2010). These studies and guidelines highlight some key design needs for people in later life: enabling the maintenance of their habitual setting with as little change as possible; maintaining rhythms and balances if a change of setting is necessary, and enabling them to continue being able to operate and learn independently. The kitchen has been found to be an environment that can enhance the quality of life for older and disabled people (Oliver, Gyi, Porter, Marshall, & Case, 2001). This study develops this work by reviewing current problems, how people manage them and offering recommendations that others could follow without necessarily redesigning the whole kitchen.
Over the life course, person-environment (P-E) interaction may change and require management through greater congruence between the two (Peace et al., 2007). One area for ergonomic guidance is to provide dimensions for the kitchen environment such as heights of worktops and shelving. For example, a survey by Ward (1971 and 1972) of kitchen worktop and sink heights, which drew from research conducted between 1943 and 1968, produced a number of recommendations. Based on her empirical research using anthropometry, electromyography and subjective preference, Ward provided recommended work heights for different activity types for 95% of British female adults. These were sink height: 90-105cm, worktop 85–100cm and cooker 85–100cm with the suggestion that 3 or 4 different height levels should be provided within each range. More recently, Kishtwaria, Mathur and Rana (2007) performed a study using physiological measures with 30 female urban homemakers in India and produced some optimum work top heights for kneading dough (79cm), chopping (84cm) and cooking (96cm). In America it is thought that the next trend will be to have taller kitchen counters (for example 42 inches or 106.7cm) to prevent the need to hunch over when handling food especially for people above average height. They would also allow for more drawer and counter space. However as Ward (1972) states, choosing a best single height does not solve the problem for individual users who may need a customized height for them, thus highlighting the need for an adjustable kitchen.
The aim of the TiKL interview study was to identify problems that older people face when using their kitchen and to identify coping strategies and practical solutions that they have created to overcome them and which could be adopted by others. A further aim was to see how these ad hoc solutions could inspire new designs for inclusive kitchens to support independent living for older people and become inclusive design features.
Method
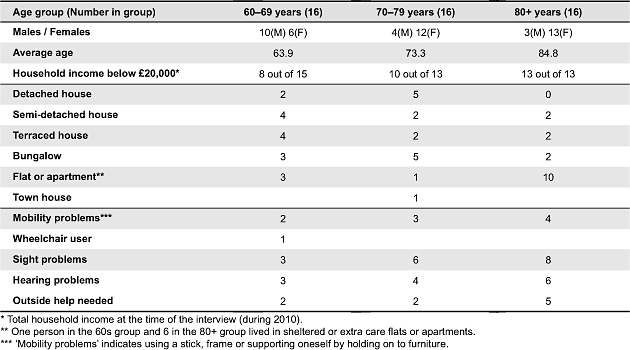
The research, conducted by social gerontologists at The Open University and ergonomists at Loughborough University involved interviewing a purposive sample of 48 older people chosen to reflect criteria relating to housing type, age group and gender. The spread of ages between those in their 60s and 90s allowed the researchers to consider temporal change in P-E fit even through cross-sectional research. An interview approach was adopted as this enabled rich and accurate data to be collected in each person’s home in a convenient manner. The information given to the participants prior to obtaining their informed consent is presented in Appendix 1. Two interviews were conducted with each person. The first was an in-depth oral history interview centred on all the kitchens they had experienced in the past, while the second focused on their current kitchen. The interviews allowed qualitative data to be collected including participants’ experiences and opinions together with photos of the current kitchen as well as quantitative data relating to kitchen activities such as ‘how often do you cook meals for yourself?’ and measurements of the size of kitchen areas, heights of shelving and worktops, and lighting levels. Participants lived in a variety of accommodation both ‘ordinary’ and ‘supportive’ in Bristol and Loughborough, England. The research did not include the care home sector where individuals in the UK do not have access to their own kitchen and meals are usually taken communally. Those participants living in ‘supportive’ housing had their own kitchen but some could eat communally if they wished (see Table 1). The research was conducted between 2009 and 2010.
Table 1. Characteristics of participants (N = 48).
Kitchen History Interview
While this paper concentrates on ‘use of’ and ‘activity within’ the contemporary kitchen for people as they age, an understanding of how past skills development and behaviour contributes to present day knowledge is also relevant. The first interview gathered an ‘oral history’ of kitchens experienced by participants during their lives. Using the oral history method (Thompson, 2000), participants were given the freedom and flexibility to recall experiences, facts and anecdotes of past kitchen life with direction by the interviewer. Prior to the interview, each person was asked to complete a table of all the houses or accommodation they had lived in including location (name of town or city), property type, approximate year moved in, approximate year when built and whether rented or owned. As dates of birth ranged from 1919 to 1948, life histories reflected societal change in the UK in the interwar and post-war periods which impacted on architectural and social experiences.
This housing history record was used to structure the interview. The interviewer used an oral history topic guide to prompt responses about kitchens and how they were used at certain life stages including: first remembered home, parental home when a teenager, leaving home and setting up first house as an independent person, having a family, and retiring. The results were of value as a record of social history. They also helped to set a context for individual participants’ preferences and feelings with regard to their current kitchens. The following quote from the study comes from an 88 year old woman currently living in Bristol. Her comments highlight issues about kitchen work and space and how her enthusiasm for cooking is recognised between the generations. This also indicates the ways in which different styles of living lead to different space standards and the need to identify places to cook. She says:
There is an amusing story because when I eventually moved to… my grandson went house hunting with my daughter, trying to find a flat for me to move into, and at one time age 4 or 5, I suppose, he went rushing around to view and he came back to his mother and said: ‘This is no good mum, this is no good’ so the woman who was showing her flat was put out, and turned to this child and said ‘What makes you say that?’. He just said ‘There is no room for granny’s marmalade’ and he had spotted at once the major fault of more modern accommodation… no storage. (Bristol participant B4, oral history)
A person’s preference for eating informally in the kitchen and using the dining room for more formal meals or when guests were present was also often reflected in the development of social etiquette across time. If a person had made small but effective adaptations to their current kitchen such as putting up extra shelves or constructing a pull out unit on wheels, they sometimes recalled past experiences of constructing kitchen storage units at a time when newly built houses might only have had basic facilities provided as standard such as a sink and draining board. When a participant commented that they felt cramped in a smaller down-sized kitchen, this was often contrasted with having a larger kitchen in a previous house. The results of the kitchen oral history work will be reported elsewhere and provide rich contextual data.
Current Kitchen Interview
Prior to the second interview, participants completed a ‘routine kitchen activities’ record detailing frequency of current kitchen use (see Appendix 2). The interview itself was semi structured (Robson, 2011) and focused on the present kitchen and how well it met the person’s abilities and needs (see Appendix 3). As noted, this paper centres on the findings from this second interview.
Each interview was carried out in the participant’s home, was directed by the researcher, and allowed time to clarify or probe particular answers. The questions in the TiKL interview considered the person’s health and well-being as well as their activities in the kitchen. It covered aspects such as physical abilities, sight, hearing, whether the person cooked, what they liked to eat. It then discussed any difficulties in completing various tasks such as cooking, washing, ironing, recycling, and feeding pets.
Following the current kitchen interview, sketches were made of the kitchen layout (see Figure 1). Photographs were taken of both good and bad features in the kitchen, identified by the participant, and any adaptations made to help improve it. Measurements were taken of the kitchen area and heights of work tops and cupboard shelves which affected how easily people could access items from them. Finally, light level measurements were taken: (1) at the kitchen sink, (2) where food was prepared, and (3) where food was eaten, for example at the kitchen table. Measurements were recorded both with the kitchen lights on and off, alongside notes of the prevailing weather conditions.
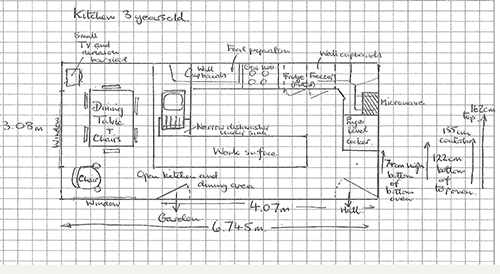
Figure 1. Example sketch of kitchen layout.
Participants were chosen to meet specific criteria. The age range was chosen to include people in their 60s through to their 90s to encompass the sociological categorizations of the ‘third ‘and ‘fourth’ ages (Baltes & Mayer, 1999; Rees-Jones et al., 2008) and to consider the impact of age on design issues. The participants were recruited across 3 age groups, 60–69, 70–79, and 80+, with 16 people in each group. There were 31 females and 17 males to reflect the different proportions in older age groups. It was also intended that they would be living in a variety of house types (detached, semi-detached, bungalow, terraced, town house, apartment or flat). Half of the sample was recruited in Bristol and half in Loughborough. Information was also gathered about their education, income, ethnic background and who else lived in the household. This ensured a range of people from different backgrounds and in different contexts. Pilot testing was done to ensure the methods to be used were appropriate. These were undertaken with 5 participants living in Loughborough, the London Borough of Haringey and Surrey, chosen to reflect the sample criteria. Full ethical approval was sought and gained from both partner institutions prior to the research being undertaken. The project team had several face-to-face meetings to plan the study, share skills and to conduct piloting for example a gerontologist leading a pilot oral history interview with an ergonomist observing, and then reversing the roles for the current kitchen interview.
Characteristics of Participant Sample
An analysis of the sample of 48 participants is shown in Table 1, divided into the three age groups.
While Table 1 shows the property types for all 48 participants, the sample included five couples, so the total number of different properties was 43. All the participants had access to their own cooking facilities. Twenty-seven participants lived on their own while 21 lived with others in the household. The ethnicity of 46 participants was ‘White British’ while 2 were ‘Asian or British Asian’. There were no apparent cultural or religious differences in terms of form and function in use of the kitchen.
Results—Past Experiences of the Kitchen
The oral histories of kitchen living were recorded and then transcribed for thematic analysis which identified a range of topics and information categories. In England, the childhood homes that many of the older participants grew up in during the 1920s and 1930s predated central heating. Typically the kitchen was the cosiest room in the house due to the presence of a coal fire or range where family members would talk, read, listen to the radio, mend clothes, bake or make jam, do homework, play board games, prepare and eat meals and do the laundry. Allied spaces, such as the scullery or utility room, were highly valued ‘back kitchen’ areas with a Belfast or Butler sink, where laundry equipment such as the copper, the wash board and the mangle might be stored and used, or where food preparation or even bathing might take place (Freeman, 2004; Goodall, 1991).
The oral histories indicate that the larder was a valuable cold walk-in space. Kitchens in which today’s older people raised their families tended to be sparsely furnished and equipped initially, but as income and family size grew, new forms of domestic equipment were obtained and valued, especially those that were labour-saving, cost-effective, and of a modern design. The kitchen has rightly been discussed as the woman’s domain but the interviews also highlighted how in the pre and post-World War 2 years, men helped by fitting work surfaces and tiles, making tables, and providing home grown or allotment produce for eating or preserving. Over time, social etiquette concerning where and how people ate their meals changed. This was reflected in features such as the ‘kitchen hatch’ linking the kitchen to the dining room, the ‘hostess trolley’, and the ‘through room’—a single lounge dining room which become a multipurpose space for leisure, social interaction and eating meals.
The kitchen remains an important hub of people’s homes, a multi-functional space where ‘things happen’, including baking, washing clothes, writing letters, having tea with a friend, and feeding the pets. Older people often find it personally rewarding to continue with familiar kitchen routines and skills known throughout their lives. This life course experience needs to be considered when discussing current kitchen form and function.
Results—Problems in the Current Kitchen, Solutions, and Strategies
Abilities Related to the Kitchen
Participants were asked about their physical or sensory abilities with respect to kitchen activities. Figure 2 shows the number of participants who had specific self-reported capability problems that caused difficulties when carrying out kitchen tasks. All category totals relate to the full sample of 48 people. It can be seen that those in the older age group (80s to 90s) tended to suffer more from impairments, particularly with sight and hearing. The participants across all groups did most of the kitchen work themselves although seven had some help from family members or a cleaner while two had more substantial help as part of caregiver visits.
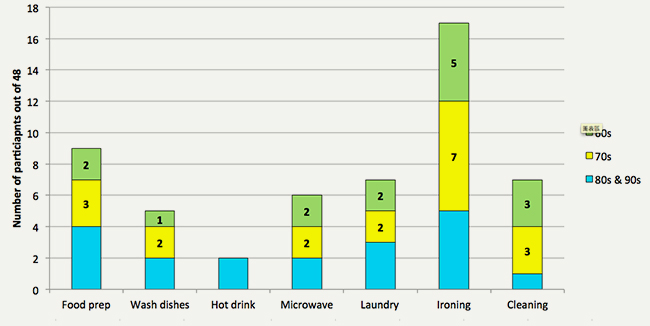
Figure 2. Number of participants in each age group experiencing specific impairments (N = 48).
Sight and Lighting
Seventeen people (35%) reported task related sight problems in the kitchen either due to a medical condition or age related. One of the most common problems was reading small instructions on food packaging or other products (6 participants) one person saying ‘They don’t want you to know’. Another common problem was in seeing the cooker or microwave display and controls clearly (4 participants) with one person finding green LED displays more difficult to read than white. Two participants cited bright sunlight as making oven or microwave controls hard to read. Another stated that when standing at the sink, the light was located behind her so was not effective.
Strategies for dealing with these problems included: using a magnifying glass or torch to help read controls or instructions on packaging (4 participants), putting on reading glasses (a hazard if leaning over hot cooker plates), using additional under cupboard lighting or a light above the cooker hob, and taking packages into the corridor where the illumination was better. One person usually got her son to help with cooker settings or a particular cooking task. Interestingly 6 of the 17 who stated they had sight problems in the kitchen did wear glasses so this was not necessarily a solution to their needs (although some may have needed their glasses updating). Participants were asked what changes they had made to help with seeing in the kitchen. Five of the households had made changes to the lighting including putting in strip lights, spotlights and under cupboard lighting. Another person had adjusted the height of their oven so it was more comfortable to view, while another had installed a talking microwave. Figure 3 shows other innovations: (i) table lamps placed on top of two wall units either side of the sink area, and (ii) a mirror located above a sink where there was no window, to reflect light from the glass panelled door opposite.

Figure 3. (1) Lamp for extra light over sink, (2) Mirror above taps to reflect light from doorway.
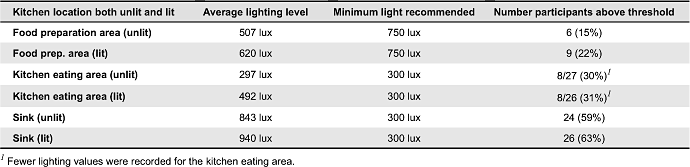
Lighting levels were measured for different areas of each kitchen in 41 of the properties including the food preparation, sink, and eating areas. Measurements were taken with and without the kitchen lights on. A considerable variation in lighting was found. Taking the recommended ergonomic lighting levels from Adams (2010), it can be seen in Table 2 that for food preparation and eating, only a minority of participants had sufficient light. As might be expected, the area near to the kitchen sink has the most light on average as this is where the kitchen window is normally located.
Table 2. Average lighting levels for kitchen areas with recommended thresholds (N = 41).
Hearing
Thirteen people (27%) reported having hearing problems. Eleven people stated that they wore a hearing aid but using it was not always straightforward, problems being: making background noises louder, not being able to raise their arm up to put it in their ear, and forgetting to wear it. For some, kitchen sounds like a boiling kettle masked the phone ringing or doorbell. Also problematic was when a person went into another room while cooking was taking place and then not hearing the kettle boil or a pan of vegetables boiling over. To cope with these problems, some participants simply kept the kitchen door open to hear what was going on if they moved into another room.
Mobility
Most people in the study could move around independently (38 or 79%). Nine (19%) needed to use a stick, frame or used furniture as support, while one was a wheelchair user. As an example of mobility needs, one 81 year old female stated that she used a trolley to transport a tray with food to the dining room or lounge. To assist with this, the fire door was taken off as it opened inwards into the kitchen which restricted space and prevented the fridge or cupboards being accessed. Although not a major factor within this study, 14 participants (29%) expressed some difficulty in using steps or stairs.
Reaching, Bending, and Posture
The ability to reach, bend down or stand for long periods of time to use appliances, cupboards, clean the floor or prepare food was a limitation for 26 people (54%). Many of the participants related problems to specific causes such as arthritis, injury, trapped nerve, dizziness or backache. Specific comments were:
…I have to crouch rather than bend to reach down to the oven so I favour my back by using my legs.
…I do not like lifting heavy items from a low position so use steps to get to higher shelves.
…I have problems reaching down. Then I have to pull myself up using the worktop.
…I can get giddy tilting my head, so it is difficult to change ceiling bulbs. The cupboards should have been lower down. The top shelf is a bit high where I put [drinking] glasses.
…You get tired standing for too long so would like a table or low work surface to sit at.
Worktop heights (measured for 26 of the kitchens) ranged from 85cm to 94cm compared to the standard kitchen countertop which is built at 90cm. One female who was 163.8cm (5 foot 4.5 inches) tall, found this work top height in her own kitchen challenging. To cope with the height of the sink, one person with a shorter stature had placed a piece of wooden board on the floor to stand on and make the sink easier to reach. The height range of the bottom shelf of each kitchen wall cupboard was also measured for 8 of the kitchens. It was found that the highest bottom shelf was 151.5cm (5 feet) from the ground and was in a kitchen owned by a woman whose height was just 157.5cm (5 foot 2 inches), approximately the same height as her eye line, making it relatively hard to reach up to the cupboard shelves.
Participants described strategies for dealing with their problems. These included using steps or a stool (5 participants), a hook or grabber to reach up to higher wall cupboard shelves or getting a son or daughter to reach up for them (3 participants). One person felt that a grabber designed with two ‘half cups’ to create a hand shape might be more effective than a simple ‘pinch’ version. Figure 4 illustrates other strategies. One participant had window handles located lower on the frame making them easier to reach, while another had new wall cupboards positioned at a lower level than standard which could also be done for existing cupboards. Some participants had installed carousel shelving to reduce the need to reach into a cupboard. One person had a small turntable placed onto a cupboard shelf to more easily access herb and spice bottles.

Figure 4. Reaching and stretching: (1) Handle at bottom of window making it easier to reach, (2) Cupboards located at a more convenient height, (3) Carousel shelf providing easier access.
An easier way to access larger items such as pans, plates and bowls is to put them into a drawer that can be pulled out without needing to reach into a cupboard. Placing a crockery rack into a drawer also makes it easier to take out individual items as needed. Lack of storage space was an issue for many people but examples were found where the available space was well utilised (see Figure 5).

Figure 5. Use of space: (1) Cup and saucer racks, (2) Additional shelving.
Strength and Dexterity
Limitations of strength and dexterity were also common within the sample, experienced by 19 participants (40%), often caused by arthritis, resulting in pain with movement and a reduction in strength. This affected many kitchen tasks such as opening jars, cans and bottles (9 participants, 19%). Common solutions reported for opening jars and other containers were to use a rubber or plastic cloth, a ring-pull opener (see Figure 6), electric tin opener, or running the jar under hot water. One person used a plastic cup or a rubber cone to grip jar lids but this only worked if they were the right size for the jar. Other problems included unscrewing the plastic top off a milk carton and pulling off the seal underneath, lifting a heavy pan or dish, and turning on taps at the sink. Two participants had special lever taps fitted which were easier to operate.

Figure 6. Rubber mat for carton opening and ring pull tin opener.
Kitchen Size, Layout, and Space
The floor areas were measured for 29 of the 43 kitchens within the study. Table 3 shows how kitchen area relates to house type and illustrates the diversity of kitchens studied. It can be seen that the 13 smallest kitchens of the 29 (45%) were located mainly in bungalows and flats. Medium to larger sized kitchens were found across a wider range of house types.
Table 3. Size of kitchen areas for part of sample (N = 29).

Nine participants mentioned layout, storage and space as reasons for liking their kitchens. Some people enjoyed having a larger space (for example “I like the natural light and amount of space”) while others preferred the benefits of a smaller area (“Not too wide for moving around” and “Kitchen nice and compact, can reach everything easily”). The problem of lack of space or poor kitchen layout was mentioned by 12 participants (25%), particularly of those living in flats or smaller houses.
The kitchen ‘work triangle’ (developed at the University of Illinois in the 1940s) is the basis of an efficiency model based on the three work centres: refrigerator, sink/dishwasher and cooker or oven (Baden-Powell, 2005). The idea is to place these three centres which form a triangle shape at the most efficient distances apart to achieve the best configuration for the space available and to minimise traffic through the work zone. The perimeter of the work triangle was measured for 18 kitchens in the sample. Kishtwaria et al. (2007) provides recommendations for kitchen layout and states that the perimeter of the work triangle should not exceed 7 metres. All 18 kitchens in the study met this requirement although a smaller triangle perimeter may be preferred if a person had mobility problems. As expected, smaller kitchens tended to contain smaller triangles while larger kitchens had larger triangles and but more flexibility in layout.
While creating an efficient layout for preparing food is a key part of an ergonomic design, other important activities are performed in the kitchen and therefore should be considered within its design. Figure 7 shows a development of the work triangle to create 3 triangles for ‘cooking’, ‘eating and clearing’, and ‘laundry’. These might be seen as a star shape—the ‘kitchen star’.
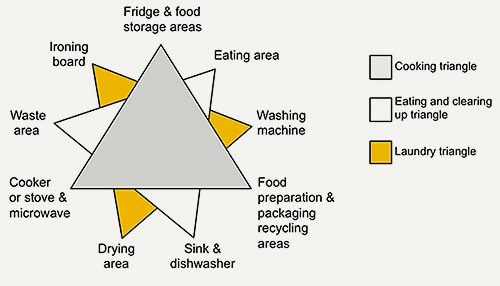
Figure 7. Adding to the traditional kitchen triangle with laundry and storage/recycling triangles.
In practice, a kitchen user will have their own patterns of movement that involve different combinations of appliances and work areas so the layout needs to be adaptable to the individual who undertakes these tasks. They will have their own personal activity map where distances between related items should be minimized or co-located. At a finer level of detail, further items could be included such as a bread bin, kettle and toaster. This could form part of a task analysis carried out to create an effective layout for a particular kitchen space. A technique for performing such an analysis in a work area is ‘link analysis’ (Robson, 2011). The kitchen star is used here as a framework for discussing the results relating to different activities.
Participants were asked if they experienced problems in performing specific tasks. Figure 8 shows the numbers who reported problems in each task category, divided by age group. These appear fairly evenly spread across the age groups for each task. Eight participants said that they received help with some tasks i.e., cleaning, making meals and gardening, either from members of the family or professional support. This included four in their 80s and 90s, two in their 70s and two in their 60s. The low number over 80 who experienced problems with cleaning may be explained by the fact that several received help with this task.
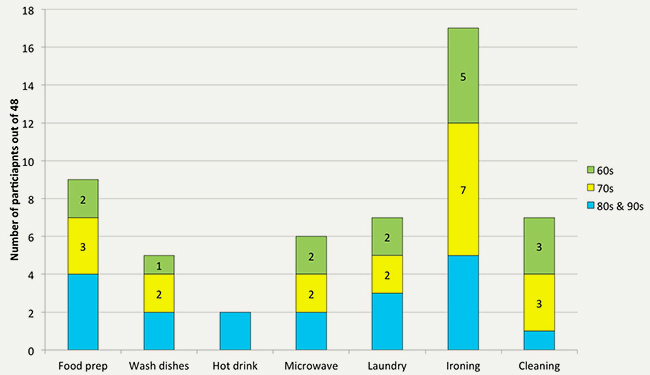
Figure 8. Numbers of participants experiencing task difficulties divided by age group.
The following sections describe these problems in more detail and any strategies employed by participants to make them easier. Specific tasks are discussed in groups relating to parts of the kitchen star.
The Cooking Triangle
Food Preparation
Nine (19%) of the 48 participants reported having problems and/or strategies for coping when preparing food. One person reported pain when peeling and chopping while another stated that her hands were not strong enough for lots of food preparation. Other participants reported problems which included backache when baking, tiredness, and standing for long periods. Some participants managed by taking short breaks between tasks while others sat down for food preparation, although this could be difficult in a small fitted galley kitchen. One lady in these circumstances spoke of liking to cook but having to sit with her knees in the opened door of the washing machine while preparing apples for chutney. Other strategies adopted to make food preparation easier included the purchase of ‘ready meals’, using a microwave oven, taking a rest break between tasks and sitting while preparing food. Further suggestions were to buy vegetables ready prepared or chopped and to steam them all in one pan. Several relied upon cooking timer devices such as the microwave ‘ping’ or a portable timer in the living room with a buzzer to warn them when cooking should be checked or was done. One said it was useful to have an auditory warning if he had fallen asleep.
Making a Hot Drink
Only three participants (6%) had difficulties making a hot drink. One found her kettle heavy and unsafe to lift and so adopted a strategy of sliding it to the tap, filling it, and then sliding it back to turn it on. Methods used, when making a hot drink, were to use a small light weight kettle or the microwave oven to heat the water in a mug. One participant said that her husband made sure there was adequate light and colour contrast between the crockery they used (cups, saucers and plates) and the work surfaces. Another option is the use of a ‘kettle tipper’, a frame in which the kettle can be placed and tipped so that water can be poured at a steady rate, with minimal risk of spillage and little effort, however, no one in the sample used this device. This may indicate a lack of awareness about some existing household aids which may only be offered by service providers to people registered as having a disability or impairment. On the other hand, many of these aids have problems of their own such as fitting the kettle in the tipping frame and removing it. Figure 9 shows how kitchen equipment can be made more accessible for people who are left-handed—a point that was commented on by some participants, although the position of the lead for a left-handed user could make using the kettle awkward to handle and potentially dangerous if it caught the lead when lifted from the stand.

Figure 9. Kettle with scales for right and left handed use.
Using a Microwave
Microwave ovens were a popular appliance with 45 (94%) of the 48 participants owning one. They were used to speed up and simplify cooking, for reheating meals, and defrosting or heating drinks. Two participants owned a combination cooker/microwave which they found useful and convenient. However six participants (12.5%) reported problems in using their microwave. These included: leaving the food cooking for too long, difficulties in transporting food from the microwave (when hot) to the work surface, having the microwave at the wrong height for convenient use, the microwave being too large for the space, and the door being on the wrong side for left handed use. Other problems were the display not being easy to see and not hearing the auditory sound or ‘ping’ when cooking was complete (due to a hearing impairment) with the meal being left standing in the microwave. It was stated that simple operation of a microwave was important, which would naturally be of benefit to users with disabilities. Two participants used an oven/microwave combination device which they found useful and convenient. One method for better cooking was to take the food out of the microwave half way through and splitting it up to make sure it was heated through properly. One woman with macular degeneration who took part in the pilot study had a raised coloured dot (a ‘bump-on’ or tactile marker) put on the microwave dial to help her set a certain heat level. This had been suggested by her local visual impairment association. Tactile markers come in various sizes, shapes and colours to help locate and operate the controls of an appliance.
The Eating and Clearing Triangle
Eating in the kitchen
Meals were eaten in the kitchen, the adjoining dining room or on a tray in the lounge. The location often depended on whether the person had company or was just eating with their partner or on their own. If there was room for a kitchen table and chair, this was found useful for kitchen tasks, eating meals and social activities. Small kitchen tables for one or two people were in use where kitchen space was limited. Another idea adopted by a participant was to have a lower work surface to sit at with space underneath for the knees, and a lower pull-out table to use when required. One person disliked breakfast bars with tall stools that required climbing onto or with insufficient leg room underneath the bar surface. A table on wheels or a trolley can be used for seated working or for moving food or utensils from the kitchen to where the meal is eaten. This is especially helpful for people with mobility problems or who cannot carry items easily.
Washing Dishes
Ten participants (21%) suffering from arthritis, reported problems with washing dishes, especially heavy items. One person used a small counter-top dishwasher (see Figure 10) while another stated that she was advised to have a more compact slim line dishwasher which fitted more easily into her kitchen. A third wanted their low level machine to be raised to a more suitable height for loading and unloading. Two stated that they loaded their dishwasher on a regular basis, and hand washed items that were not too dirty. To help with manual washing up, participants suggested adopting a routine of washing the dishes just once a day to make the activity more efficient, and using a drainer to save on drying up.

Figure 10. (1) Small countertop dishwasher, (2) Slimline dishwasher.
Waste Disposal and Recycling
All participants did recycling and split items into the various bags or containers provided by the local council. Most had a waste bin in the kitchen and many had a designated space for storing items for recycling such as a kitchen worktop, fridge top, cupboard, or in plastic bags or boxes. Problems included: difficulty bending or moving to empty pedal bins and not knowing in which bags to put different items of waste or recycling. To overcome these difficulties, one solution was to place the rubbish bin on a bench and lift the lid manually. Waste or recycling bags also have to be carried to an external shared container or put in a bin and moved to the roadside on collection day which some people found difficult.
Feeding pets
Eight participants had pets that they fed or looked after in the kitchen (six cats, one budgerigar and one spaniel dog). No specific problems were reported. Most kept the pet food in the kitchen. One strategy for managing pet food was to buy and keep food in bulk in the garage and to bring in small amounts as needed. Also available are adjustable height feeding bowls, saving the owner from having to bend down to floor level and the older pet from having to stretch his or her neck to reach the food. Figure 11 shows a raised dog feeder containing two bowls.

Figure 11. Elevated pet bowl so there is less bending for pet and owner.
Cleaning
Seven participants (15%) had problems cleaning their kitchen. They were from the younger and middle aged groups indicating that the oldest participants had assistance. Problems included: being able to move an appliance forward to clean behind it, bending to clean the oven and fridge, cleaning from a wheelchair, reaching to clean the windows and vacuuming the kitchen carpet. ‘Common sense’ suggestions for cleaning the freezer included running down items and doing the defrosting on a cold day so that food temporarily located outside of the freezer did not warm up too quickly.
The Laundry Triangle
Washing Clothes
Seven participants (15%) reported having problems with washing and drying clothes. Comments from participants indicated a desire for outdoor drying that could be problematic for flat dwellers. Participants commented:
…I have a rotary line which I leave up but closed (folded down) with a cover on to keep it clean.
…I prefer to dry clothes outside but carrying them onto the patio is difficult so I shuffle the basket with my feet.
…My drying machine is difficult to open and close as the door is heavy to lift into and out of the (locking) socket.
One person living in a low rise flat reported that she had to race downstairs if the clothes were hanging outside when it rained, and one couple said how much they missed hanging out washing when they moved to a flat.
Twenty four participants described their methods for managing the household washing and drying which included: washing small amounts at a time; sending larger items to the laundry; doing the washing in the afternoon and drying with heaters overnight; and using radiators or a clothes horse for drying in a warm area such as the conservatory. Several participants valued their tumble dryers for getting their washing dry and leaving it warm. Some people in sheltered accommodation had a shared laundry facility while another couple used a commercial laundry. One person with visual impairment used assistive tactile markers attached to the washing machine to help locate the controls.
Ironing
Seventeen participants (35%), 10 women and 7 men, reported having problems with ironing—this task causing the most difficulty in the sample. Specific problems included managing a heavy ironing board and lifting and carrying it to a suitable location. Strategies adopted to make the task easier were to only use the ironing board for large items and using a kitchen work top for others, using a lighter board, and limiting ironing to the main items (not underwear or sheets). Visiting relatives also helped with ironing. Of the 31 participants who did not experience problems with ironing, interestingly no-one did the ironing in the kitchen, indicating that they may have avoided any problems by moving the task to where there was more space. For example, they may have a spare room where they could leave the ironing board up. Another solution is to install a small pull out ironing board that can fold down or slot into a work surface in the kitchen. No one reported having this facility but several participants had a peninsula worktop or a pull out table that could act as an ironing surface if covered by a cloth.
Likes, Dislikes, and Changes
Participants were asked what aspects of their kitchen they most liked or disliked. The results are summarized in Table 4 with the frequency of responses shown in brackets:
Table 4. Likes and dislikes relating to the current kitchen.
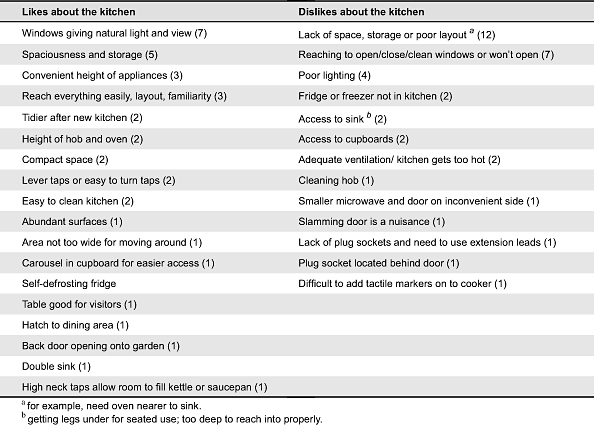
There were few obvious differences between the kinds of problems experienced by people across the different age groups. More space was a requirement for all groups and it was apparent that several of those who had moved from a larger house to a flat or apartment found the smaller kitchen restricting. Regarding the problem of reaching windows or windows not opening, this affected one person in their 60s, two in their 70s and four in their 80s and 90s, indicating that the older age group tend to experience problems with these kinds of physical tasks to a greater degree.
People were asked what changes or additions they had made in their kitchen. These included:
- Appliances: more plug sockets or better positioning; obtaining a dishwasher, automatic kettle, lighter iron, water filter tap, lever taps and new radiators.
- Environment: a light that can be lowered over the kitchen table; under or over or cupboard lighting; a mirror above the sink to reflect light from a glass panelled door, giving a view to the garden when washing up.
- Storage: additional cupboards (where space allowed); pull out shelves in cupboards.
- Cleaning: lighter colour flooring to show dirt; vinyl off-cuts on top of wall units so they can be removed and cleaned.
- Reaching and access: pull out shelves in cupboards; corner cupboards with revolving units for access.
- General: specially designed kitchen to meet needs (installed or planned).
There were few clear differences between solutions adopted by the different age groups. Two participants in their 60s and two in their 70s had extended or had a new kitchen installed. None of the participants in their 80s or 90s had plans for this. One person stated that their kitchen had been updated with new tiles and cupboards but they did not want to knock walls down or make major changes. There was some evidence that the younger participants were more aware about newer kitchen fittings on the market and appliances that could make the kitchen easier to use than the older participants, some of whom thought they would like to make improvements but were not always sure how they could be achieved.
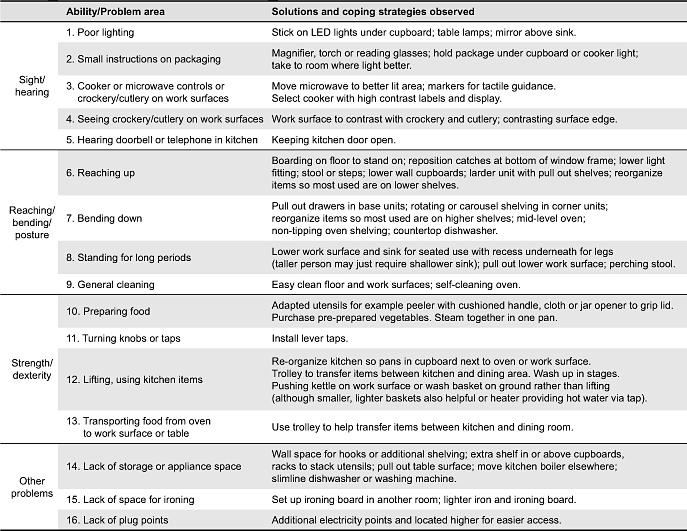
Summary of Solutions and Strategies
Table 5 lists the different solutions or coping strategies for managing to problems in the kitchen that were identified during the study.
Table 5. Summary table of kitchen solutions.
Discussion
Employing Design Solutions
The research has highlighted many ergonomics problems that older people currently face. Many people were seen to be coping with their problems but not making changes to their kitchens that could give a better longer term solution. For example:
- Using a stool or grabber to reach high shelves or into awkward cabinets rather than having lower or carousel cupboards.
- Managing with a floor level oven rather than a mid-level oven.
- Continuing to wash up rather than having a slimline dishwasher installed into a small kitchen.
- Taking frequent rests from standing rather than having a lower level worktop or table to sit at.
- Managing with a microwave rather than having a malfunctioning cooker replaced.
- Unhappy with old sink but reluctant to change it.
Understandably many people experience feelings of inertia about making changes to their kitchen. It may be felt to be too troublesome and expensive and so they may just put up with the way it is or with appliances that do not work. This matches the belief that older people tend to be more resistant to change (Westerhoff, 2008). However when changes are made people may experience less disruption than they expect, as one participant found when he had a new boiler installed:
…I sat in this chair and their organisation was fantastic. They came in at twenty to eight in the morning and put six radiators in, all the pipe work, took the old one out and they were gone at two o’clock. Blimey.... I can switch it on and off and within a quarter of an hour it’s warm.
Sometimes a lack of knowledge when making adaptions created further problems. For example, in one bungalow an extra drawer had been fitted at floor level below the lower drawer of a base unit, to give more space. While this provided extra space it was difficult for the user to bend down far enough to access it. In another kitchen, a wooden board had been put on the floor for the person to stand on to help reach the sink. However the lack of a contrasting edge to the board meant that it was a possible tripping hazard. When presenting similar ideas to householders there is also a need to offer supplementary advice and warnings to ensure that they are safe as well as effective.
Lack of kitchen space and poor layout was a recurring theme within the study. A continuing goal for kitchen design is therefore the provision of storage space at a convenient height for access and an optimum layout for the given kitchen space. This involves keeping appliances located close enough together to save effort of movement and in a way that avoids awkward twisting for people with reduced mobility. Although larger kitchens give more space for units, equipment and an optimum layout, smaller more compact designs normally require less movement to carry out everyday tasks.
All the ideas and innovations adopted by participants to overcome problems in the kitchen have been compiled into a booklet (Maguire et al., 2012) and distributed to consumers, kitchen designers and installers.
Applicability of the Study Results beyond the UK
The TiKL study was based on kitchens installed in a diverse range of UK properties constructed throughout the 20th century and traditionally comprising a sink, refrigerator/freezer and integrated cooker or separate oven and hob. Each kitchen contained a washing machine which in some of the larger properties was located within a utility room also containing drying facilities. Although kitchen designs may vary between countries, it is likely that many of the tasks, ergonomic problems and proposed solutions will be relevant to other countries. For example Kishtwaria et al. (2007) conducted research that related to a sample of Indian people performing the tasks of chopping vegetables, cooking vegetables, kneading dough and dishwashing – the same as would be performed in the UK and kitchens worldwide. Johansson Lundberg & Borrell (2011) performed a study which identified key principles for the design of kitchens in Scandinavia for older people with cognitive impairments. The principles that the authors identified included: (a) safety; (b) support for order and structure; (c) simplicity of function and use; and (d) guidance through recognition and intuition. The TiKL study is very much about how people in later life perform physical activities and use their senses to interact with the kitchen furniture and its equipment. Clearly there are synergies between the findings and recommendations from all three studies which imply that the results of the TiKL project would be useful beyond the UK.
The following sections are reflections on the research methodology used in the TiKL project which may be of benefit to others conducting similar user-centred studies.
Interview Preparation
In conducting interviews with older people, particularly those who have not participated in a similar study, it was found that having a discussion beforehand helps to reassure people that they could usefully take part. For those in poorer health, flexibility is required in posing fewer questions, focusing on key topics and cutting down on the formalities of the study. This approach helped put participants at their ease and was important for a successful interview. It also facilitated follow-up visits, when required, to fill in any gaps in the information collected.
The approach of collecting the kitchen history for each participant helped to set the context for how they viewed their current kitchen. So, for example, if they had been used to a larger family kitchen previously they would perhaps feel less content with a smaller kitchen having downsized to move into a smaller property. Also by forewarning them about the content of the interview, this gave the participants a chance to think in advance about any problems within their kitchen which could then be discussed as well as any solutions or innovations they wished to talk about.
Taking Pictures, Making Sketches and Light Measurements
When participants were asked if they would like to take pictures of the kitchen environment using digital cameras provided by the research team, many preferred the researcher to take pictures of particular features for them. However there may be a need for participants to take pictures outside of the interview of problems with performing kitchen tasks. Here a simple digital camera should be selected to minimize the difficulties a participant may have in using it. When the picture files were later stored on computer, it was found useful to give each one an explanatory name for easy reference during the analysis for example ‘Well organized storage cupboard’ and ‘LED light attached to shelf’. Making sketches of the whole kitchen formed a good basis for recording kitchen dimensions. It was found helpful to take the light readings with the participant standing in their normal working positions in the kitchen to give a more realistic measure of the light falling in each work area.
The Need for Satisfaction Ratings and Benefit of Direct Observations
One feature of the study that would have been useful to include was a rating of how satisfied each person was with their own kitchen or how serious they considered each problem to be. This would have helped to set the findings in context and prioritise the need for solutions to particular problems. A small number of video recordings were made (in addition to the main study) where some of the participants talked about and demonstrated their use of the kitchen. With more time it would have been interesting to observe or record participants carrying out one or more kitchen tasks to identify kitchen features they had not considered problematic. It was also important to be aware that participants would occasionally say that they had no problems with a particular task and then reported the difficulties they had. Consequently it is necessary to record all comments made as people engage with the kitchen space, alongside managing the more structured interview format.
Recommendations
The following is a summary of the solutions employed by kitchen users, designers and installers which can help to make kitchens a friendlier environment for older users.
Ensuring Enough Light and Instruction Visibility
The study has shown that many kitchens have insufficient light in specific task areas such as where food is prepared and where it is eaten. Traditionally windows are placed above a sink to allow people to look outside while working. Consideration should also be given to allowing natural light to fall on a work surface (perhaps adjoining the sink) as a natural place to perform preparation tasks where light is needed. Under cupboard lighting can also be installed where the light fittings can be hidden by the rim. Lighting design should also take account of how easily people can renew bulbs so that they are not left unchanged when the bulb or tube fails. Having light fittings that can be lowered from the ceiling to replace a bulb would help many people who cannot reach up to change a bulb or use steps. The installation of automatic task lighting above a work surface which activates when a person is in proximity to it is also beneficial. People may install their own table lamps in a kitchen so sufficient electrical sockets above the work surfaces would help facilitate this. Problems in reading small instructions on packaging are a nuisance for many people. Magnifiers and spare reading glasses were used to help with this. A magnifier with an integrated light could be installed on a flexible arm, at a suitable point, to help read small print. When appliances are installed in a kitchen, the person choosing them should try and consider how easily the controls and labels will be seen in the kitchen environment rather than a brightly lit showroom.
Providing Easier Access and More Storage
Kitchen storage design has progressed to facilitate easier access for people with mobility problems. Examples include larder units with open sides which can be pulled out and accessed more easily, deeper drawers that can support the weight of plates, pans and bowls, and carousel storage options to maximize space in smaller kitchens. Installing extra shelves is also a way to create space in the kitchen to display valued crockery, cookbooks, or herbs and spices. Incorporating hooks and holders into a kitchen design is also a way to save space, allowing kitchen towels, mugs and utensils to be hung up. Providing ovens and other appliances at mid-level also offers easier access in many kitchens and adopting this as a standard configuration would make the kitchen more usable for people who find it hard to bend down to reach inside an oven. Having a heat-proof pull out worktop next to the oven would also provide a surface for transferring a pan to and from the oven. For one oven product, the door can be pulled down and slid underneath the oven space so that it is out of the way, making it easier to access.
Adjustable wall cupboards are also available that can be pulled down and forward to more easily reach items. Having at least one unit of this type installed in a standard kitchen would be helpful for many people. Much can also be achieved by storing items commonly used in the most convenient locations, with heavy items being stored at hip and shoulder height to avoid over-stretching. Items should also be stored as close as possible to the place they’ll be used. Having pull out features in a kitchen such as a pull out table top (at sitting height) or ironing surface (for standing) are valuable for people who do not have the space for a kitchen table or ironing board. Being able to work in a seated position at a table or lower work surface also avoids having to stand for long periods when preparing food. Having some open storage also makes items easier to access without having to open a cupboard door especially if in a wheelchair. Glass-fronted cupboards and/or open shelves are a helpful way of coping when a person’s memory isn’t as good as it was. The glass in the cupboards also reflects light, helping to make the kitchen brighter. Folding aluminium kitchen steps with a grip that is usable with both hands are best for kitchen users of all ages. They are light, easily moved, and in width when folded, don’t take any more room to store than steps without a grip. A socket outlet in the floor allows an ironing board or swing out table-leaf easier access to the power source. This allows more cable for the iron or kitchen appliance and prevents it from trailing across a working surface, or impeding movement round the kitchen. However, it does involve bending to connect plug to the power and to remove it.

Figure 12. (1) Glass fronted and open cupboards, (2) Safe steps, (3) Socket outlet in the floor.
Addressing Problems of Strength and Dexterity
In the study, many people reported difficulties in lifting heavy pans and kettles and in opening jars and turning taps. Lighter utensils are therefore beneficial. Kettles with a gauge helps prevent overfilling while lightweight pans requiring less strength should be considered. When the kitchen is installed, fitting lever taps or taps with easy-turn heads makes them more accessible for all occupants and saves them being retrofitted. The problem of opening jars has been well researched and new designs to assist those with arthritis and similar conditions are always appearing. Using a pedal bin can be awkward for many people and so hands free bins have been developed that self-open when approached using infrared sensor technology. Such bins may also have a manual button press option to open them.
More Flexible Kitchens
Modern fully fitted kitchens are likely to be harder to modify than the more modular kitchens from the past. An interesting finding from the study was that several people were reluctant to make changes to their kitchens because they thought it would be too difficult and costly. One aspect of the modern fitted kitchen is that it is less easy to change specific units without needing to replace the whole kitchen. While fitted kitchens benefit from having a continuous worktop area that makes them easier to work on and keep clean, there is also a place for free standing units such as a drawer unit, kitchen dresser or sideboard with drawers and shelves for storing crockery, cutlery and tableware. These provide extra storage and flexibility so they can be moved or replaced when required. As Sims et al. (2012a) states:
…Putting separate items such as the ‘kitchen cupboard’ and multipurpose items back in the kitchen, as part of a range of separate units that together form a modular adaptable kitchen, may present a more sustainable solution for kitchen design.
Bespoke Kitchens
The design of bespoke kitchens is one way to achieve more inclusive kitchens by allowing the customer to specify worktop, base unit and cupboard dimensions for their particular height and reach, and to take account of any particular disabilities they may have. So for example a person in a wheelchair would require sink and worktops that are set at a lower height and are usable from a seated position and for cupboards and shelving to be open to save having to manoeuvre around doors. If DIY and kitchen stores could offer more choice of sizes, for example three heights of worktop, this would lead to kitchens matching user needs more closely. These options could be built in kitchen planning software. If a higher work surface is needed, a way to achieve this without affecting resale house value is to use standard base cabinets and adding a piece of wood under the counter top that can be taken out without disturbing the cabinetry.
Conclusions
The kitchen project was composed of researchers from different disciplines which has been both helpful and stimulating. The social gerontological researchers introduced the approach of oral history to capture information from participants using a housing history and topic guide in a way that was not over directed. The ergonomists were able to bring their knowledge of a more structured approach to capture people’s abilities, task activities, problems and opinions of the current kitchen so that both qualitative and quantitative findings could be drawn out and assembled in a consistent format.
The methodology used in this study emphasizes the importance of understanding the users, their characteristics, the environment in which they are living and working and the tasks they are carrying out. It is recommended that in order to create a kitchen environment to enhance the quality of people’s lives, the chosen approach should consider these aspects. This may include interviews of people in their homes, observing them performing typical tasks or even asking them to keep a diary of their day-to-day activities and problems in the kitchen.
The study has identified a number of ergonomic issues and problems relating to contemporary kitchen use by older people and explored the coping strategies and adaptations made to overcome them as shown in Table 5. Many of these problems are not new. In comparing the results of a kitchen study conducted in 2000 with those from the TiKL project in 2010, it appears that only limited progress has been made in terms of kitchen design to meet the needs of older people (Sims et al., 2012b). Yet there are now a wider range of more suitable kitchen units on the market and it is partly a matter of advising consumers about what is available and how to better organize their kitchens to help make them easier to use. This type of information has been used to create a guide The easier kitchen: Making it happen (Maguire et al, 2012) for use by consumers, designers and manufacturers. A copy of this guide and further information about the project can be obtained from the authors or the project website: www.lifelongkitchens.org
There are other potential solutions to ergonomic problems in the kitchen beyond those observed in the study, based on smart technologies. These include motorized cupboards and work surfaces that can be raised and lowered, a scanner for reading out small text on packaging, and the ability for appliances such as irons and ovens to automatically switch off when the person leaves the house—see for example, Design Matters (2010), BBC (2011) and Maguire et al. (2011). However for such technological solutions to be accepted, they have to be seen as useful, feasible, and simple to operate.
A further challenge is to recognize the importance of the kitchen in enabling older people to stay within their own home for as long as possible. There is a need to think in terms of kitchens that are more flexible and able to be adapted to meet people’s needs at different life stages particularly as they grow older. These may be thought of as ‘democratic kitchens’ that take on board the needs and concerns of all people, giving them an equal say in future kitchen design. The kitchen that accommodates the needs of people as they get older should be a kitchen that meets the needs of all age-groups.
Acknowledgement
The authors would like to thank the New Dynamics of Ageing programme in the UK for sponsoring the Transitions in Kitchen Living project and all the participants who welcomed us into their homes and kitchens during the study. We are also grateful to the project advisory committee and the older people’s research group representatives, Mary Sinfield and Theresa LeFort, for their useful advice throughout the project.
References
- Adams, C. (2010). About.com: Kitchen ergonomics: Lighting levels by room. Retrieved August, 2013, from http://ergonomics.about.com/od/lighting/a/lightlevelrooms.htm
- Baden-Powell, C. (2005). Architect’s pocket book of kitchen design. Oxford, UK: Architectural Press.
- Baltes, P. B., & Mayer, K. U. (Eds.) (1999). The Berlin aging study: Aging from 70 to 100. New York, NY: Cambridge University Press.
- BBC (2011). ‘Smart’ kitchen appliances connect to web. Retrieved August, 2013, from http://news.bbc.co.uk/1/hi/programmes/click_online/9362154.stm
- Câmera, J. J. D. (2010). Analysis and ergonomics of houses for elderly people. Periodicum Biologorum, 112(1), 47-50.
- Design matters (2010). Designer’s tour of kitchen tailored for disabled people. Retrieved August, 2013, from http://www.bbc.co.uk/news/uk-11893452
- Freeman, J. (2004). The making of the modern kitchen: A cultural history. Oxford, UK/New York, NY: Berg.
- Goodall, P. (1991). Design and gender: Where is the heart of the home? Built Environment 16(4), 269-278.
- Huppert, F. (2003). Designing for older users. In J. Clarkson, R. Coleman, S. Keates, & C. Lebbon (Eds.), Inclusive design: Design for the whole population (pp. 30-49). London, UK: Springer-Verlag.
- Johansson, K., Lundberg, S., & Borrell, L. (2011). “The cognitive kitchen”–Key principles and suggestions for design that includes older adults with cognitive impairments as kitchen users. Technology and Disability, 23(1), 29-40.
- Kishtwaria, J., Mathur, P., & Rana, A. (2007). Ergonomic evaluation of kitchen work with reference to space designing. Journal of Human Ecology, 21(1), 43-46.
- Lin, S. (2008). Designing for the senior surge, makers of appliances, bath fixtures target aging boomers; cooking for the forgetful. The Wall Street Journal (online). Retrieved August, 2013, from http://www.smarthomesolutions.com/pdfs/DesigningfortheSeniorSurge.pdf
- Maguire, M., Nicolle, C., Marshall, R., Sims, R., Lawton, C., Peace, S., & Percival, J. (2011). A Study of user needs for the ‘techno kitchen’. In C. Stephanidis (Ed.), Proceedings of the International Conference on HCI (Posters, Part II, pp. 66-71). Heidelberg, Germany: Springer.
- Maguire, M., Peace, S., Marshall, R., Nicolle, C., Percival, J., and Sims, R., (2012). The easier kitchen: Making it happen, transitions in kitchen living project, new dynamics of ageing Programme. Milton Keynes, UK: The Open University.
- Moore, L. J., & Ostrander, E. R. (1992). In support of mobility: Kitchen design for independent older adults. New York, NY: Cornell Cooperative Extension. Retrieved August, 2013, from http://ecommons.cornell.edu/handle/1813/3329
- Odén, B., Beck-Friis, B., & Östlund, B. (2010). Elderly people and design. Lund, Sweden: Lund University. Retrieved August, 2013, from http://www1.design.lth.se/aldreochdesign/elderlypeopleanddesign_screen.pdf
- Oliver, R. E., Gyi, D. E., Porter, J. M., Marshall, R., & Case, K. (2001). A Survey of the design needs of older and disabled people. In M. A. Hanson (Ed.),Contemporary ergonomics (pp. 365-370). Cirencester, UK: Taylor & Francis.
- Peace, S., Wahl, H-W., Mollenkopf, H., & Oswald, F. (2007). Environment and Ageing. In J. Bond, S. Peace, F. Dittman-Kohli, & G. Westerhof (Eds.), Ageing in society: European perspectives in gerontology (pp. 209-234). London, UK: Sage Publications.
- Rees-Jones, I., Hyde, M., Victor, C. R., Wiggins, R. D., Gilleard, C., & Higgs, P. (2008). The Historical Evolution of the Third Age. Ageing in a consumer society: From passive to active consumption in Britain (pp.13-28). Bristol, UK: The Policy Press.
- Robson, C. (2011). Real world research (3rd Ed.). Chichester, UK: John Wiley and Sons Ltd.
- Sims, R.E., Marshall, R., Maguire, M., Nicolle, C., Lawton, C., Peace, S., & Percival, J. (2012a). Design of kitchens for independence: Lessons from history for the future. In: M. Anderson (Ed.), Contemporary ergonomics and human factors 2012, (pp. 39-46), London, UK: Taylor and Francis.
- Sims, R. E., Maguire, M. C., Nicolle, C., Marshall, R., Lawton, C., Peace, S., & Percival, J. (2012b). Older people’s experiences of their kitchens: 2000 to 2010. Housing, Care and Support, 15(1), 6-15.
- Thomas Pocklington Trust (2010). Good practice guide No 4: Housing for people with sight loss - A practical guide to improving existing homes. Retrieved August, 2013, from http://www.pocklington-trust.org.uk/news/news/news_channels/research/gpg4
- Thompson, P. R. (2000). The voice of the past: Oral history (3rd ed.), Oxford, UK: Oxford University Press.
- Ward, J. (1971). Ergonomics techniques in the determination of optimum work surface heights. Applied Ergonomics, 2(3), 171-177.
- Ward, J. (1972). Ergonomics in the kitchen, The Design Journal, October 1972, 58-59. Retrieved August, 2013, from the Online Resource for the Visual Arts. http://vads.ac.uk/diad/article.php?title=286&year=1972&article=d.286.34
- Westerhoff, N. (2008). Set in our ways: Why change is so hard, Scientific American, December 17, 2008.
Appendix
Appendix 1: Participant information
An information sheet was created for distribution to the participants prior to obtaining their consent to take part in the study. It contained the following elements:
Purpose of the Study
- To examine the experience of the kitchen in later life for people living in a variety of accommodation both mainstream and supportive housing.
- Details of the project partners and sponsors.
Method
- Study based on 48 people living in a range of accommodation in Bristol and Loughborough.
- Two interviews to be carried out in the participant’s home, the first on the different kitchens that they have experienced in their lives, and the second about their current kitchen and how it fits their needs.
- Each interview would last for about one and half hours and be audio recorded.
- Photos would be taken of the current kitchen to highlight particular problems or interesting features, a sketch made of the kitchen layout and some measurements taken.
- Forms would be completed by the participant to collect some background details about the person, routine kitchen activities, and a list of all the houses lived in, to guide the kitchen history interview.
- The person would be given a small token of thanks for taking part in the research and, if they wished, a copy of the interview recording or photos for their own records.
Planned Outcome
- The project will develop a resource for other researchers, based on the interview data and a practical guide to help people design or adapt their kitchens for easier use.
Storage of Data
- All interview transcripts will be stored securely and only submitted to the UK Research Council’s research resource in anonymized form.
Right to withdraw
- The participant has the right to withdraw from the study at any time.
Appendix 2: Routine kitchen activities
The participant was asked to write down activities which generally happen at the following times of day:
- Breakfast time/early morning
- Mid-morning
- Lunchtime
- Mid-afternoon
- Dinner time/early evening
For example: ‘Breakfast: Get the mugs, cereal and bread out of the breakfast cupboard and the orange juice and the spread from the fridge’. They were also asked to record the times when each activity normally started.
Appendix 3: Interview structure
The current kitchen interview was based on the following questions.
Abilities and problems
- 1. Whether the person could move around the home unaided or whether they required a walking aid, used furniture to aid movement, or were a wheelchair user.
- 2. Problems with steps or stairs.
- 3. Problems accessing the kitchen.
- 4. Difficulties with sight, for example, reading the settings on the cooker or weights on the scales. Changes made or coping strategies used to address vision or lighting problems.
- 5. Difficulties with hearing for example, the kettle boiling or a saucepan overheating, and strategies to help manage these problems.
Cooking and diet
- 6. The person was asked if they cooked meals for themselves, how often and at what times of day. If not, how meals were provided.
- 7. Did the person eat meals in the kitchen, elsewhere or both.
- 8. The kinds of food preferred.
- 9. Whether the person had lost any weight over the last 6 months.
- 10. Rating of own current health and effect on kitchen activities.
Personal characteristics and problems with specific activities
- 11. The person’s height.
- 12. If right or left handed.
- 13. Problems with the following actions:
- Reaching above the head, bending down or reaching forward
- Dexterity, co-ordination or strength in the hands or wrists
- Preparing food and cooking meals
- Washing up or loading and unloading the dishwasher
- Making a hot drink
- Using the microwave
- Washing and drying clothes.
Waste disposal and recycling
- 14. Where rubbish or waste packaging is kept.
- 15. Whether recycling takes place and how it is done.
- 16. Whether ironing is done in the kitchen and location of ironing board.
Pets
- 17. Whether pets are fed in the kitchen.
- 18. Problems in looking after pets related to the kitchen.
Cleaning
- 19. Problems with kitchen cleaning, for example, physical actions, hard-to-reach places.
Other topics
- 20. Help received with kitchen tasks and to what extent.
- 21. Likes or dislikes about the kitchen.
- 22. Changes made to kitchen.
- 23. Whether the design or layout has been influenced by ideas from elsewhere, for example, a restaurant, school or hospital kitchen, showroom, exhibition, or TV programme.
- 24. Other activities in the kitchen not covered, for example, watching TV, listening to the radio, coffee mornings or family events.
